
 PDF下载 ( 3395 KB)
PDF下载 ( 3395 KB)

不同评分模型对肝硬化患者经颈静脉肝内门体分流术后生存的预测价值
DOI: 10.3969/j.issn.1001-5256.2023.03.016
Value of different scoring models in predicting the survival of patients with liver cirrhosis after transjugular intrahepatic portosystemic shunt
-
摘要:
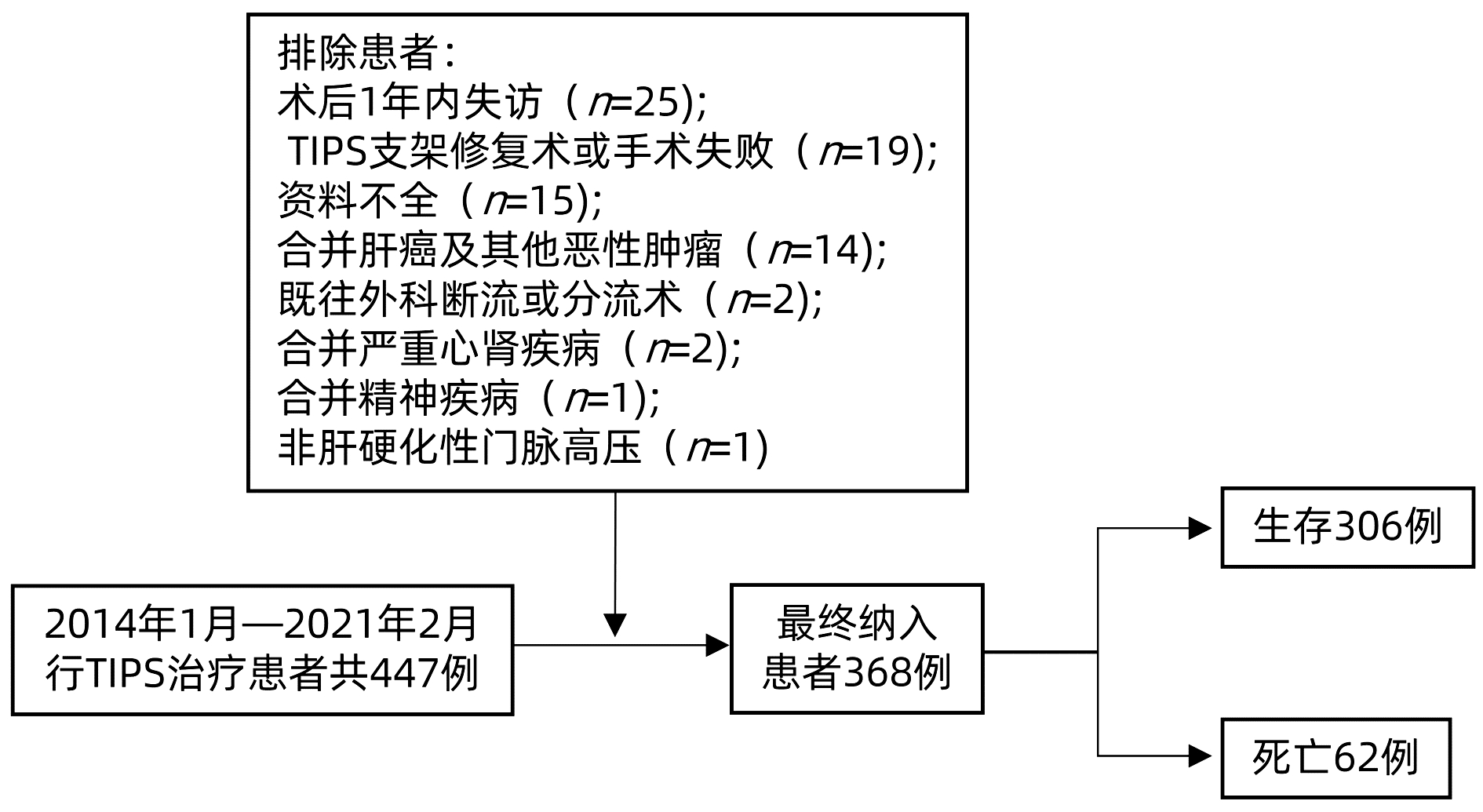
目的 探讨Child-Pugh评分、终末期肝病模型(MELD)评分、联合血清钠离子的终末期肝病模型(MELD-Na)评分、慢性肝衰竭联盟-急性失代偿(CLIF-C AD)评分和经颈静脉肝内门体分流术(TIPS)术后生存Freiburg指数(FIPS)评分对肝硬化患者生存的预测价值。 方法 回顾性分析2014年1月—2021年2月我国西南地区多家医院行TIPS治疗的447例肝硬化患者的临床资料,其中生存组306例,死亡组62例。计算五种评分模型分值,并基于五种评分模型分别对患者进行生存分析。正态分布的计量资料组间比较采用独立样本的t检验;不符合正态分布的计量资料组间比较采用非参数Mann-Whitney U检验;计数资料组间比较采用Pearson χ2检验;采用Cox回归分析各评分模型对TIPS患者预后的影响;Kaplan-Meier法分析不同评分水平的患者死亡风险的差异,并采用Log-rank检验。各模型预测能力采用受试者工作特征曲线下面积(AUC)、不同时间点C指数及决策曲线进行评估。 结果 生存组患者年龄(Z=2.884)低于死亡组,Alb(t=3.577)、Na+(Z=-3.756)均高于死亡组,而酒精性肝硬化患者比例(χ2=22.674)、AST(Z=2.141)、PT(Z=2.486)、INR(Z=2.429)、TBil(Z=3.754)、腹水严重程度(χ2=14.186)及五种模型评分均低于死亡组(P值均<0.05)。生存分析显示,各评分模型均能有效对TIPS患者预后进行风险分层。对各评分模型不同时间点C指数比较发现,Child-Pugh评分对术后生存预测能力较高,其次为MELD-Na评分、MELD评分和CLIF-C AD评分,而FIPS评分预测能力相对较差,此外,随时间延长,各评分预测效能均减弱。Child-Pugh评分术后1年生存率的预测效能最大(AUC=0.832),MELD-Na评分术后3年生存率的预测效能最大(AUC=0.726),而FIPS评分术后在1年和3年生存预测能力比较中均较差。 结论 五种评分模型均可作为肝硬化TIPS术后患者生存的预测方法,且都可为肝硬化TIPS患者提供有效的预后风险分层。在短期预测上Child-Pugh评分生存预测能力更好,长期预测上MELD-Na评分生存预测能力更好,而FIPS评分预测能力均相对较差。 -
关键词:
- 肝硬化 /
- 门静脉高压 /
- 门体分流术, 经颈静脉肝内
Abstract:Objective To compare the value of Child-Pugh score, Model for End-Stage Liver Disease (MELD) score, MELD combined with serum sodium concentration (MELD-Na) score, CLIF Consortium Acute Decompensation (CLIF-C AD) score, and Freiburg index of post-transjugular intrahepatic portosystemic shunt (TIPS) survival (FIPS) score in predicting the survival of patients undergoing TIPS. Methods A retrospective analysis was performed for the clinical data of 447 patients with liver cirrhosis who underwent TIPS in several hospitals in southwest China, among whom there were 306 patients in the survival group and 62 in the death group. The scores of the above five models were calculated, and a survival analysis was performed based on these models. The independent samples t-test was used for comparison of normally distributed continuous data between groups, and the non-parametric Mann-Whitney U test was used for comparison of non-normally distributed continuous data between groups; the Pearson chi-square test was used for comparison of categorical data between groups; a multivariate Cox regression analysis was used for correction analysis of known influencing factors with statistical significance which were not included in the scoring models; the Kaplan-Meier method was used to evaluate the discriminatory ability of each model in identifying risks in the surgical population, and the log-rank test was used for analysis. The area under the receiver operating characteristic curve (AUC), C-index at different time points, and calibration curve were used to evaluate the predictive ability of each scoring model. Results Compared with the death group, the survival group had significantly lower age (Z=2.884, P < 0.05), higher albumin (t=3.577, P < 0.05), and Na+ (Z=-3.756, P < 0.05) and significantly lower proportion of patients with alcoholic cirrhosis (χ2=22.674, P < 0.05), aspartate aminotransferase (Z=2.141, P < 0.05), prothrombin time (Z=2.486, P < 0.05), international normalized ratio (Z=2.429, P < 0.05), total bilirubin (Z=3.754, P < 0.05), severity of ascites (χ2=14.186, P < 0.05), and scores of the five models (all P < 0.05). Survival analysis showed that all scoring models effectively stratified the prognostic risk of the patients undergoing TIPS. Comparison of the C-index of each scoring model at different time points showed that Child-Pugh score had the strongest ability in predicting postoperative survival, followed by MELD-Na score, MELD score, and CLIF-C AD score, and FIPS score had a relatively poor predictive ability; in addition, the prediction efficiency of each score gradually decreased over time. Child-Pugh score had the largest AUC of 0.832 in predicting 1-year survival rate after surgery, and MELD-Na score had the largest AUC of 0.726 in predicting 3-year survival rate after surgery, but FIPS score had a poor ability in predicting 1- and 3-year survival rates. Conclusion All five scoring models can predict the survival of patients with liver cirrhosis after TIPS and can provide effective stratification of prognostic risk for such patients. Child-Pugh score has a better ability in predicting short-term survival, while MELD-Na score has a better ability in predicting long-term survival, but FIPS score has a relatively poor predictive ability in predicting both short-term and long-term survival. -

注:a, 校正年龄、肝硬化病因和Na+后,Child-Pugh评分是TIPS患者预后的独立影响因素;b, 校正年龄、腹水、Alb和Na+后,MELD评分是TIPS患者预后的独立影响因素;c, 校正年龄、腹水和Alb后,MELD-Na评分是TIPS患者预后的独立影响因素;d, 校正肝硬化病因、腹水、Alb和TBil后,CLIF-C AD评分是TIPS患者预后的独立影响因素;e, 校正肝硬化病因、腹水、和Na+后,FIPS评分是TIPS患者预后的独立影响因素。
图 2 各评分模型多因素Cox回归分析森林图
Figure 2. Forest plot of multifactor Cox regression analysis for each scoring model
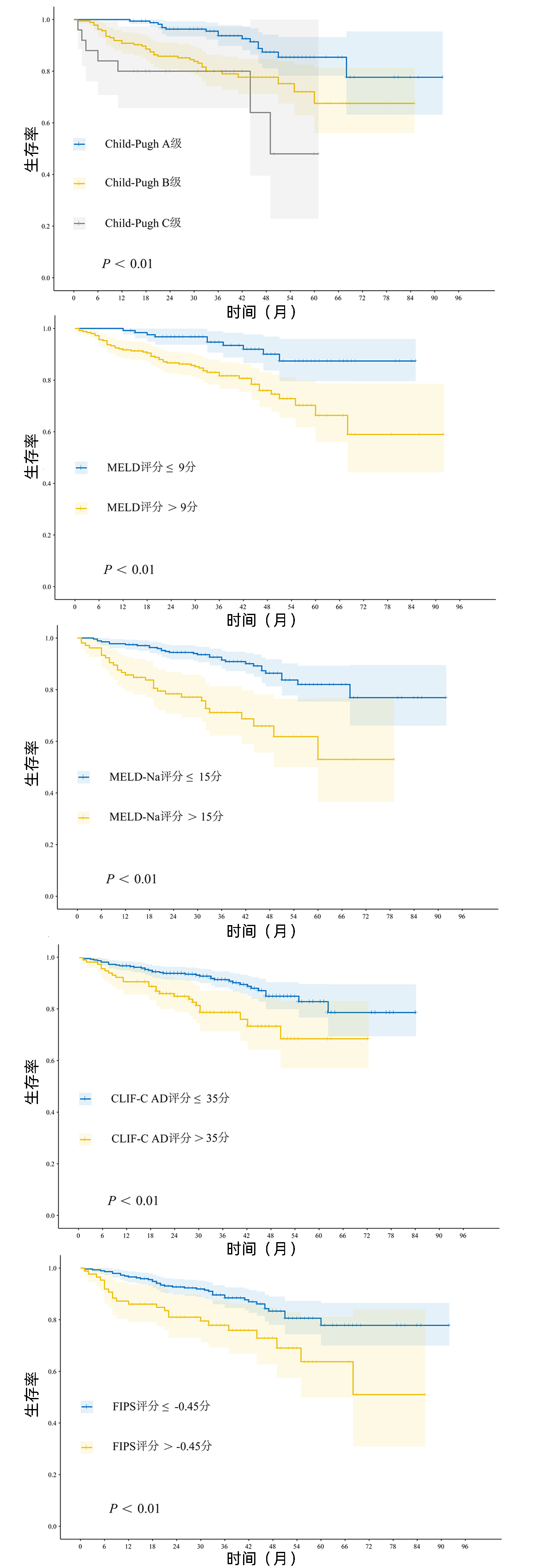
图 3 各评分模型内不同风险亚组患者生存曲线
Figure 3. Survival curves of patients in different risk subgroups within each scoring model

注:a, C指数;b, 决策曲线;c, 术后1年ROC曲线;d, 术后3年ROC曲线。
图 4 各评分模型预测能力的比较
Figure 4. Comparison of prediction ability of each scoring model
表 1 368例肝硬化患者临床资料基线特征
Table 1. Baseline characteristics of clinical data of 386 patients with liver cirrhosis
指标 所有患者(n=368) 生存组(n=306) 死亡组(n=62) 统计值 P值 年龄(岁) 52(45~60) 50(45~59) 56(49~66) Z=2.884 0.004 性别[例(%)] χ2=2.378 0.123 男性 263(70.9) 214(69.3) 49(79.0) 女性 105(29.1) 92(30.7) 13(21.0) BMI(kg/m2) 22.9(21.0~24.9) 22.9(21.1-25.0) 22.7(20.8~24.7) Z=-0.230 0.818 术前PVP(cmH2O) 34(29~36) 34(30~36) 32(29~35) Z=0.194 0.153 术后PVP(cmH2O) 20(19~21) 20(19~20) 20(18~20) Z=0.657 0.657 肝硬化病因[例(%)] χ2=22.674 <0.001 病毒性 267(71.4) 235(75.3) 32(51.6) 酒精性 42(11.9) 24(8.5) 18(29.0) 其他 59(16.7) 47(16.1) 12(19.4) 腹水量[例(%)] χ2=14.186 0.001 无 155(41.8) 141(45.6) 14(22.6) 轻度 101(27.5) 83(27.2) 18(29.0) 中-重度 112(30.7) 82(27.2) 30(48.4) WBC(×109/L) 3.67(2.50~5.60) 3.59(2.49~5.54) 4.02(2.86~5.62) Z=1.260 0.208 Hb(g/L) 83.0(68.5~100.0) 83.0(69.0~100.0) 82.0(68.0~106.0) Z=-0.406 0.685 PLT(×109/L) 61(43~90) 60(43~89) 61(43~101) Z=1.030 0.303 Alb(g/L) 35.0±6.1 35.6±6.1 32.3±5.3 t=3.577 <0.001 AST(U/L) 34.3(25.6~50.9) 33.7(25.3~47.6) 38.9(27.6~63.2) Z=2.141 0.032 ALT(U/L) 26.3(18.8~38.1) 26.6(19.2~37.6) 22.5(16.3~41.9) Z=-0.252 0.801 TBil(μmol/L) 24.4(17.9~33.8) 23.1(16.7~31.9) 29.5(22.5~49.3) Z=3.754 <0.001 Scr(μmol/L) 68.2(57.7~78.7) 68.3(58.0~77.1) 66.9(54.9~82.8) Z=0.331 0.741 PT(s) 13.7(12.6~15.3) 13.6(12.5~14.9) 14.6(13.0~16.4) Z=2.486 0.011 INR 1.19(1.09~1.33) 1.18(1.09~1.29) 1.29(1.13~1.43) Z=2.429 0.015 Na+(mmol/L) 138.5(136.4~140.3) 138.9(137.2~140.4) 137.0(134.2~139.0) Z=-3.756 <0.001 Child-Pugh评分 7(6~8) 7(6~8) 8(7~9) Z=4.374 <0.001 MELD评分 10.2(8.4~12.1) 9.9(8.2~11.8) 11.3(9.8~14.6) Z=-1.077 <0.001 MELD-Na评分 12.4(10.6~14.4) 12.2(10.4~13.8) 14.3(12.0~16.6) Z=0.378 <0.001 CLIF-C AD评分 38.8(34.8~45.1) 38.3(34.3~44.5) 42.9(37.3~47.4) Z=3.356 0.001 FIPS评分 -0.91(-1.35~-0.47) -0.96(-1.40~-0.54) -0.62(-1.00~-0.06) Z=3.613 <0.001 注:PVP,门静脉压。  下载: 导出CSV
下载: 导出CSV
表 2 单因素Cox回归分析结果
Table 2. Univariable Cox regression analysis for prognostic factors
项目 OR(95%CI) P值 项目 OR(95%CI) P值 年龄 1.047(1.022~1.072) <0.001 PLT 1.003(0.999~1.006) 0.185 BMI 0.982(0.907~1.063) 0.647 Alb 0.924(0.888~0.961) <0.001 性别 0.655(0.355~1.208) 0.176 AST 1.001(0.997~1.006) 0.562 PVP ALT 0.998(0.992~1.005) 0.633 术前 0.976(0.924~1.030) 0.373 TBil 1.029(1.018~1.040) <0.001 术后 0.967(0.892~1.050) 0.426 Scr 1.002(0.990~1.013) 0.764 病因(病毒性比照) PT 1.168(1.054~1.294) 0.003 酒精性 3.990(2.238~7.116) <0.001 INR 5.561(1.721~17.977) 0.004 其他 1.823(0.937~3.546) 0.077 Na+ 0.907(0.863~0.953) <0.001 腹水(无腹水比照) Child-Pugh评分 1.490(1.290~1.721) <0.001 轻度 2.096(1.042~4.216) 0.038 MELD评分 1.199(1.116~1.288) <0.001 中重度 3.865(2.043~7.314) <0.001 MELD-Na评分 1.195(1.122~1.273) <0.001 WBC 1.102(0.943~1.085) 0.748 CLIF-C AD评分 1.079(1.044~1.116) <0.001 Hb 0.998(0.988~1.009) 0.738 FIPS评分 2.168(1.495~3.144) <0.001
下载: 导出CSV
-
[1] BOIKE JR, THORNBURG BG, ASRANI SK, et al. North American practice-based recommendations for transjugular intrahepatic portosystemic shunts in portal hypertension[J]. Clin Gastroenterol Hepatol, 2022, 20(8): 1636-1662.e36. DOI: 10.1016/j.cgh.2021.07.018. [2] Chinese College of Interventionalists. CCI clinical practice guidelines: management of TIPS for portal hypertension (2019 edition)[J]. J Clin Hepatol, 2019, 35(12): 2694-2699. DOI: 10.3969/j.issn.1001-5256.2019.12.010.中国医师协会介入医师分会. 中国门静脉高压经颈静脉肝内门体分流术临床实践指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2694-2699. DOI: 10.3969/j.issn.1001-5256.2019.12.010. [3] LIU F, ZHAO JB, WANG JY, et al. Transjugular intrahepatic portosystemic shunt via jugular vein by using specialized covered stent: 2-year follow-up observation[J]. J Interv Radiol, 2021, 30: 888-892. DOI: 10.3969/j.issn.1008-794X.2021.09.007. [4] PUGH RN, MURRAY-LYON IM, DAWSON JL, et al. Transection of the oesophagus for bleeding oesophageal varices[J]. Br J Surg, 1973, 60: 646-649. DOI: 10.1002/bjs.1800600817. [5] MALINCHOC M, KAMATH PS, GORDON FD, et al. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts[J]. Hepatology, 2000, 31(4): 864-871. DOI: 10.1053/he.2000.5852. [6] BIGGINS SW, KIM WR, TERRAULT NA, et al. Evidence-based incorporation of serum sodium concentration into MELD[J]. Gastroenterology, 2006, 130(6): 1652-1660. DOI: 10.1053/j.gastro.2006.02.010. [7] JALAN R, PAVESI M, SALIBA F, et al. The CLIF Consortium Acute Decompensation score (CLIF-C ADs) for prognosis of hospitalised cirrhotic patients without acute-on-chronic liver failure[J]. J Hepatol, 2015, 62(4): 831-840. DOI: 10.1016/j.jhep.2014.11.012. [8] BETTINGER D, STURM L, PFAFF L, et al. Refining prediction of survival after TIPS with the novel Freiburg index of post-TIPS survival[J]. J Hepatol, 2021, 74(6): 1362-1372. DOI: 10.1016/j.jhep.2021.01.023. [9] de FRANCHIS R, BOSCH J, GARCIA-TSAO G, et al. Baveno Ⅶ - Renewing consensus in portal hypertension[J]. J Hepatol, 2022, 76(4): 959-974. DOI: 10.1016/j.jhep.2021.12.022. [10] COLAPINTO RF, STRONELL RD, BIRCH SJ, et al. Creation of an intrahepatic portosystemic shunt with a Grüntzig balloon catheter[J]. Can Med Assoc J, 1982, 126(3): 267-268. [11] GIANNINI E, BOTTA F, FUMAGALLI A, et al. Can inclusion of serum creatinine values improve the Child-Turcotte-Pugh score and challenge the prognostic yield of the model for end-stage liver disease score in the short-term prognostic assessment of cirrhotic patients?[J]. Liver Int, 2004, 24(5): 465-470. DOI: 10.1111/j.1478-3231.2004.0949.x. [12] HUO TI, WANG YW, YANG YY, et al. Model for end-stage liver disease score to serum sodium ratio index as a prognostic predictor and its correlation with portal pressure in patients with liver cirrhosis[J]. Liver Int, 2007, 27(4): 498-506. DOI: 10.1111/j.1478-3231.2007.01445.x. [13] RUBIN RA, HASKAL ZJ, O'BRIEN CB, et al. Transjugular intrahepatic portosystemic shunting: decreased survival for patients with high APACHE Ⅱ scores[J]. Am J Gastroenterol, 1995, 90(4): 556-563. [14] PARVINIAN A, SHAH KD, COUTURE PM, et al. Older patient age may predict early mortality after transjugular intrahepatic portosystemic shunt creation in individuals at intermediate risk[J]. J Vasc Interv Radiol, 2013, 24(7): 941-946. DOI: 10.1016/j.jvir.2013.03.018. [15] FENG IC, TZENG WS, WANG SJ, et al. The role of transjugular intrahepatic portosystemic shunt in acute variceal bleeding: differential survival owing to different cirrhosis etiology[J]. J Gastroenterol, 2010, 27: 166-174. DOI: 10.6557/GJT.201006_27(2)0.0001 [16] SAAD N, RUDE MK, DARCY M, et al. Older age is associated with increased early mortality after transjugular intrahepatic portosystemic shunt[J]. Ann Hepatol, 2016, 15(2): 215-221. DOI: 10.5604/16652681.1193716. [17] LI J, TANG S, ZHAO J, et al. Long-term survival prediction for transjugular intrahepatic portosystemic shunt in severe cirrhotic ascites: assessment of ten prognostic models[J]. Eur J Gastroenterol Hepatol, 2021, 33(12): 1547-1555. DOI: 10.1097/MEG.0000000000001890. [18] ASCHA M, ABUQAYYAS S, HANOUNEH I, et al. Predictors of mortality after transjugular portosystemic shunt[J]. World J Hepatol, 2016, 8(11): 520-529. DOI: 10.4254/wjh.v8.i11.520. [19] WEN L, HE S, ZHANG H, LUO X. Comparison study of five scoring systems for evaluating prognosis of patients undergoing transjugular intrahepatic portosystemic shunt procedures[J]. Chin J Hepatol, 2014, 22: 514-518. DOI: 10.3760/cma.j.issn.1007-3418.2014.07.008 .文龙跃, 何松, 张浩, 等. 五种评分系统对经颈静脉肝内门体静脉分流术患者预后的评价比较[J]. 中华肝脏病杂志, 2014, 22: 514-518. DOI:10.3760/cma.j.issn.1007-3418.2014.07.008 .[20] SCHEPKE M, ROTH F, FIMMERS R, et al. Comparison of MELD, Child-Pugh, and Emory model for the prediction of survival in patients undergoing transjugular intrahepatic portosystemic shunting[J]. Am J Gastroenterol, 2003, 98(5): 1167-1174. DOI: 10.1111/j.1572-0241.2003.07515.x. [21] ANGERMAYR B, CEJNA M, KARNEL F, et al. Child-Pugh versus MELD score in predicting survival in patients undergoing transjugular intrahepatic portosystemic shunt[J]. Gut, 2003, 52(6): 879-885. DOI: 10.1136/gut.52.6.879. [22] YANG C, CHEN Q, ZHOU C, et al. FIPS score for prediction of survival after TIPS placement: External validation and comparison with traditional risk scores in a cohort of chinese patients with cirrhosis[J]. AJR Am J Roentgenol, 2022, 219(2): 255-267. DOI: 10.2214/AJR.21.27301. [23] LV Y, WANG Z, LI K, et al. Risk stratification based on chronic liver failure consortium acute decompensation score in patients with child-pugh B cirrhosis and acute variceal bleeding[J]. Hepatology, 2021, 73(4): 1478-1493. DOI: 10.1002/hep.31478. -

 本文二维码
本文二维码
计量
- 文章访问数: 851
- HTML全文浏览量: 344
- PDF下载量: 123
- 被引次数: 0

