
 PDF下载 ( 2045 KB)
PDF下载 ( 2045 KB)

脾体积对肝硬化门静脉高压性胃病及其严重程度的预测价值
DOI: 10.3969/j.issn.1001-5256.2023.04.013
Value of spleen volume in predicting portal hypertensive gastropathy and its severity in patients with liver cirrhosis
-
摘要:
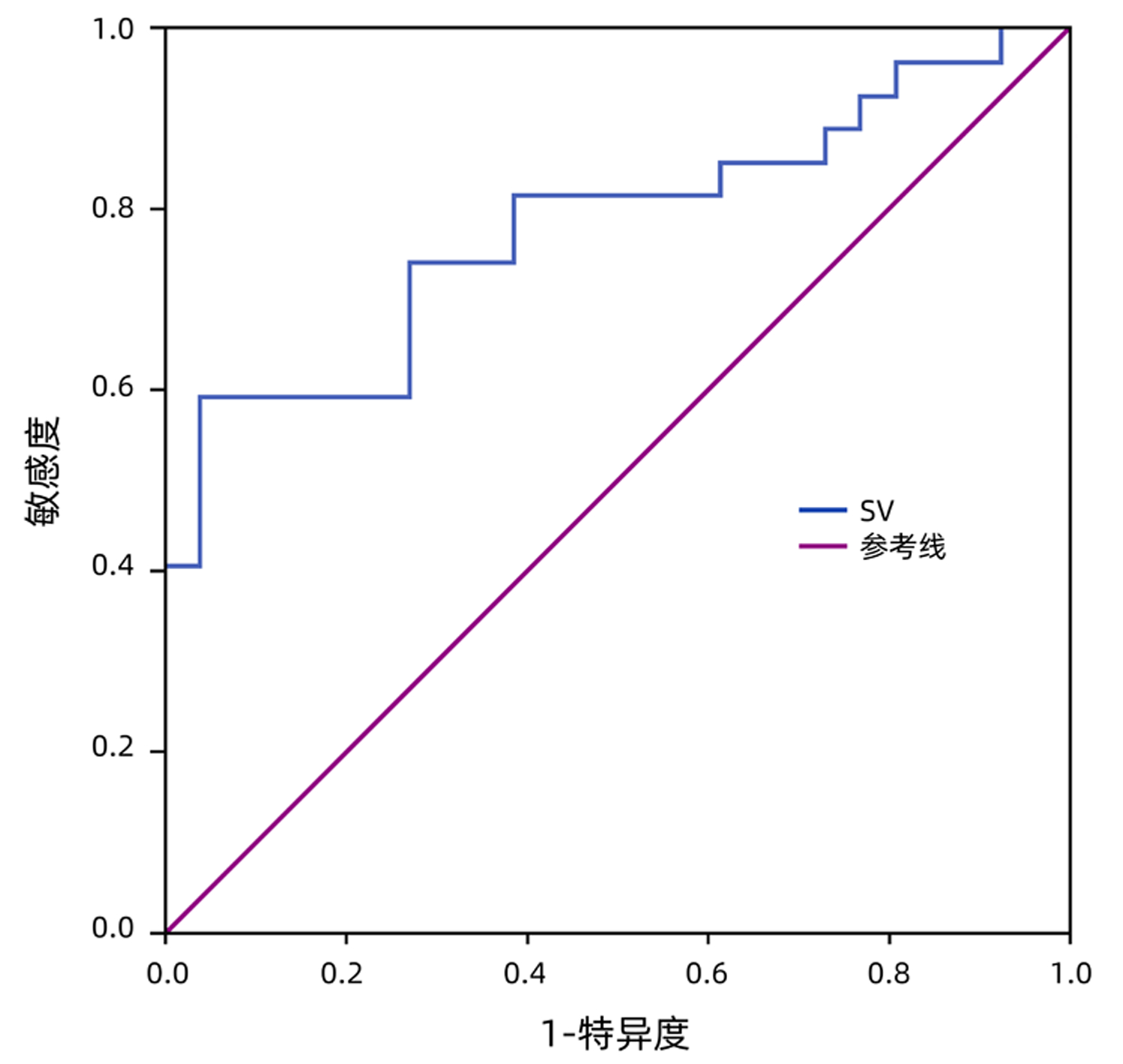
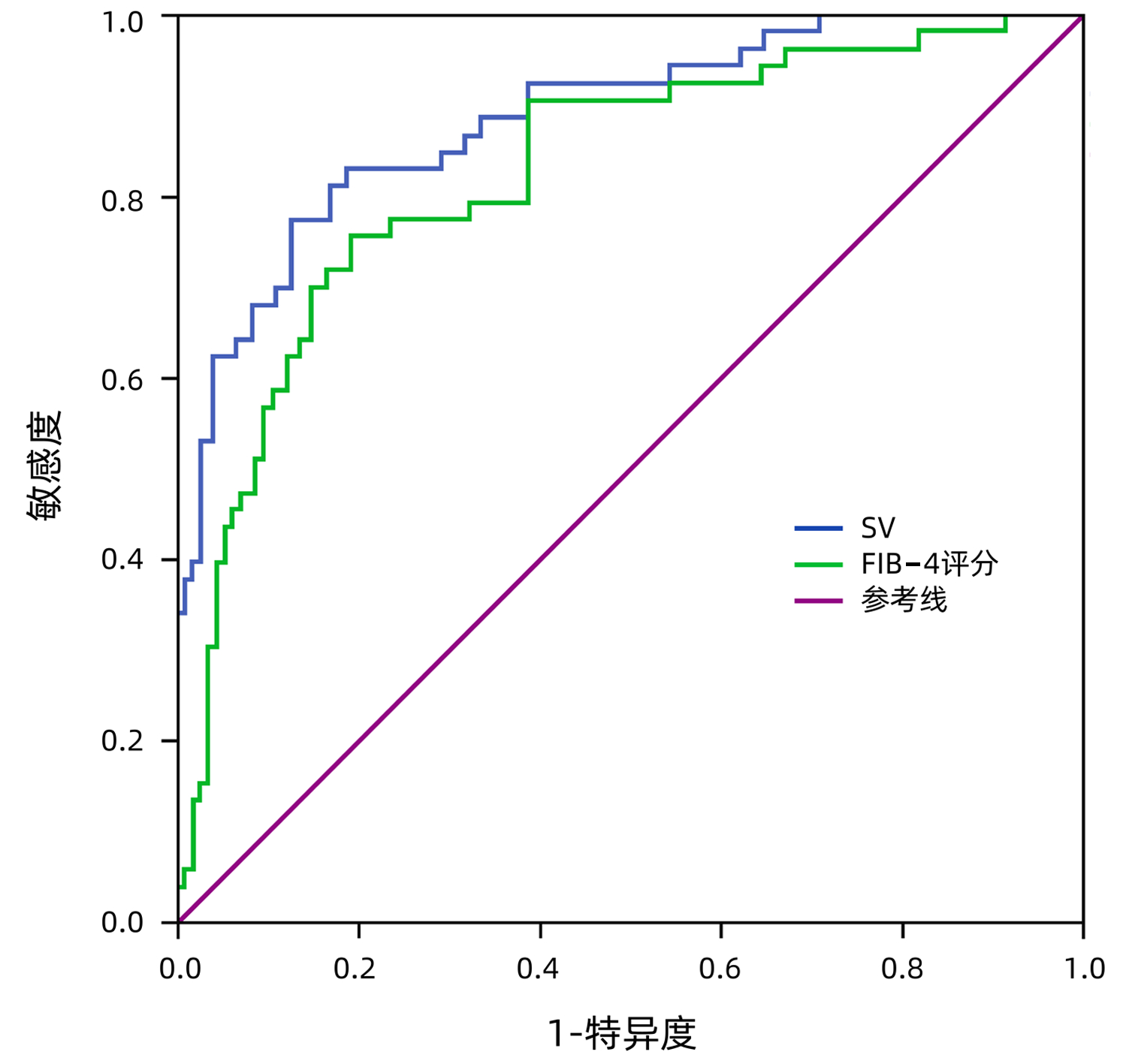
目的 探讨脾体积(SV)对肝硬化患者门静脉高压性胃病(PHG)及重度PHG的预测价值。 方法 回顾性分析2018年1月—2022年8月湖北医药学院附属襄阳市第一人民医院收治的168例肝硬化患者临床资料,以胃镜检查结果为“金标准”,将患者分为无PHG组(n=115)和PHG组(n=53),轻度PHG组(n=26)和重度PHG组(n=27),所有患者均行电子胃镜、腹部磁共振及相关血清学检查,获取相关指标及参数。正态分布的计量资料两组间比较采用成组t检验;非正态分布的计量资料两组间比较采用Mann-Whitney U检验。计数资料两组间比较采用χ2检验。通过多因素Logistic回归分析筛选出PHG、重度PHG的独立危险因素,利用受试者工作特征曲线(ROC曲线)比较相关指标或参数的预测价值。ROC曲线下面积的比较采用Delong检验。 结果 单因素分析显示:PHG组和非PHG组性别、有无腹水、Hb、PLT、AST、TBil、Alb、PT、INR、Child-Pugh分级、FIB-4评分、King评分、Lok评分、脾长径(SD)、SV、血小板/脾长径(PSDR)、血小板/脾体积(PSVR)比较,差异均有统计学意义(P值均<0.05);轻度PHG组和重度PHG组Hb、PLT、Alb、SD、SV、PSDR、PSVR比较,差异均有统计学意义(P值均<0.05)。多因素Logistic回归分析显示:FIB-4评分(OR=1.280,95%CI:1.009~1.625)和SV(OR=1.007,95%CI:1.001~1.013)是PHG发生的独立危险因素(P值均<0.05);SV(OR=0.990,95%CI:0.980~1.000)是重度PHG发生的独立影响因素(P<0.05)。ROC曲线分析结果显示:在预测PHG发生时,SV的曲线下面积为0.884, 高于FIB-4评分的0.825(P<0.05),其最佳临界值为406.82,敏感度为0.774,特异度为0.870;在预测重度PHG发生时,SV的曲线下面积为0.782,最佳临界值为714.63,敏感度为0.593,特异度为0.962。 结论 SV对PHG和重度PHG的发生均具有较好的预测价值。 Abstract:Objective To investigate the value of spleen volume (SV) in predicting portal hypertensive gastropathy (PHG) and severe PHG in patients with liver cirrhosis. Methods A retrospective analysis was performed for the clinical data of 168 patients with liver cirrhosis who were admitted to Xiangyang No.1 People's Hospistal Affiliated to Hubei University of Medicine from January 2018 to August 2022, and with the results of gastroscopy as the gold standard, these patients were divided into non-PHG group with 115 patients and PHG group with 53 patients; the PHG group was further divided into mild PHG group with 26 patients and severe PHG group with 27 patients. All patients underwent electronic gastroscopy, abdominal magnetic resonance imaging, and serological examination to obtain related indices and parameters. The group t-test was used for comparison of normally distributed continuous data between two groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test was used for comparison of categorical data between two groups. A multivariate Logistic regression analysis was used to screen out the independent risk factors for PHG and severe PHG, and the receiver operating characteristic (ROC) curve was used to compare the predictive value of related indices or parameters. The area under the Roccurve is compared using Delong test. Results The univariate analysis showed that there were significant differences between the PHG group and the non-PHG group in sex, presence or absence of ascites, hemoglobin (Hb), platelet count (PLT), aspartate aminotransferase, total bilirubin, albumin (Alb), prothrombin time, international normalized ratio, Child-Pugh class, FIB-4 score, King score, Lok score, spleen diameter (SD), SV, platelet count/spleen diameter ratio (PSDR), and platelet count/spleen volume ratio (PSVR) (all P < 0.05), and there were significant differences in Hb, PLT, Alb, SD, SV, PSDR, and PSVR between the mild PHG group and the severe PHG group (all P < 0.05). The multivariate Logistic regression analysis showed that FIB-4 score (odds ratio [OR]=1.280, 95% confidence interval [CI]: 1.009-1.625, P < 0.05) and SV (OR=1.007, 95% CI: 1.001-1.013, P < 0.05) were independent risk factors for PHG, and SV (OR=0.990, 95% CI: 0.980-1.000, P < 0.05) was an independent influencing factor for severe PHG. The ROC curve analysis showed that in predicting PHG, SV had a larger area under the ROC curve (AUC) than FIB-4 score (0.884 vs 0.825, P < 0.05), with a sensitivity of 0.774 and a specificity of 0.870 at the optimal cut-off value of 406.82; in predicting the onset of severe PHG, SV had an AUC of 0.782, with a sensitivity of 0.593 and a specificity of 0.962 at the optimal cut-off value of 714.63. Conclusion SV has a good value in predicting the onset of PHG and severe PHG. -
Key words:
- Liver Cirrhosis /
- Portal Hypertensive Gastropathy /
- Forecasting
-
表 1 无PHG组与PHG组一般资料比较
Table 1. General information of patients in No-PHG group and PHG group
变量 无PHG组(n=115) PHG组(n=53) 统计值 P值 性别(男/女,例) 65/50 41/12 χ2=6.765 0.009 年龄(岁) 54.79±10.74 51.65±11.38 t=-1.709 0.089 吸烟史(有/无,例) 35/80 21/32 χ2=1.378 0.240 饮酒史(有/无,例) 34/81 23/30 χ2=3.096 0.078 高血压史(有/无,例) 28/87 6/47 χ2=3.814 0.051 病因(例) χ2=3.767 0.052 乙型肝炎 74 42 其他 41 11 腹水(有/无,例) 31/84 34/19 χ2=21.159 <0.001 Hb(g/L) 137.10±19.81 119.64±25.59 t=-4.395 <0.001 PLT(×109/L) 148.00(109.00~192.00) 65.00(53.50~101.00) Z=-7.951 <0.001 ALT(U/L) 27.70(17.70~60.00) 27.40(21.55~52.45) Z=-0.486 0.627 AST(U/L) 33.40(26.10~54.90) 45.20(33.40~61.35) Z=-2.483 0.013 TBil(μmol/L) 18.24(15.20~28.30) 25.79(18.64~39.16) Z=-3.301 0.001 Alb(g/L) 42.47±5.74 37.87±6.43 t=-4.644 <0.001 PT(s) 11.00(10.50~11.60) 12.10(11.65~13.35) Z=-5.864 <0.001 INR 0.94(0.91~1.00) 1.06(1.02~1.16) Z=-5.982 <0.001 Child-Pugh分级(例) χ2=12.546 0.002 A级 95 30 B级 17 20 C级 3 3 FIB-4评分 2.54(1.75~3.77) 6.09(3.94~8.63) Z=-6.763 <0.001 King评分 13.41(8.08~30.67) 37.48(22.69~53.98) Z=-5.497 <0.001 Lok评分 -0.16(-0.96~0.39) 1.30(0.51~2.13) Z=-6.900 <0.001 SD(mm) 111.63±22.43 152.07±29.12 t=8.959 <0.001 SV(cm3) 240.79±138.25 597.30±275.86 t=8.907 <0.001 PSDR(n·cm-3·mm-1) 1 304.43(978.24~1 875.26) 452.46(319.40~675.63) Z=-8.330 <0.001 PSVR(n·cm-3·cm-3) 749.88(438.72~1 185.13) 132.26(69.53~215.77) Z= -8.477 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 轻度PHG组与重度PHG组一般资料比较
Table 2. General information of patients in Mild PHG group and Severe PHG group
变量 轻度PHG组(n=26) 重度PHG组(n=27) 统计值 P值 性别(男/女,例) 18/8 23/4 χ2=1.925 0.165 年龄(岁) 52.12±12.31 51.33±9.90 t=-0.255 0.800 吸烟史(有/无,例) 12/14 9/18 χ2=0.910 0.340 饮酒史(有/无,例) 14/12 10/17 χ2=1.510 0.219 高血压病史(有/无,例) 2/24 4/23 χ2=0.148 0.701 病因(例) 乙型肝炎 19 23 χ2=1.181 0.277 其他 7 4 腹水(有/无,例) 15/11 19/8 χ2=0.926 0.336 Hb(g/L) 111.62±26.92 127.37±22.06 t=2.334 0.024 PLT(×109/L) 83.50(62.00~114.25) 56.00(51.00~71.00) Z=-3.194 0.001 ALT(U/L) 23.65(19.63~46.85) 35.10(25.00~53.10) Z=-1.406 0.160 AST(U/L) 47.16(32.28~89.48) 41.60(37.80~49.30) Z=-1.076 0.282 TBil(μmol/L) 23.15(17.70~32.90) 30.20(21.98~46.20) Z=-1.779 0.075 Alb(g/L) 35.99±6.27 39.67±6.17 t=2.156 0.036 PT(s) 11.95(11.30~12.33) 12.60(11.80~13.40) Z=-0.962 0.336 INR 1.05(1.02~1.16) 1.09(1.02~1.17) Z=-0.695 0.487 Child-Pugh分级(例) χ2=0.555 0.912 A级 14 16 B级 10 10 C级 2 1 FIB-4评分 5.48(3.14~10.39) 6.12(4.70~7.57) Z=-0.071 0.943 King评分 29.68(18.03~97.45) 47.01(31.97~52.17) Z=-1.050 0.294 Lok评分 1.42(0.53~2.31) 1.14(0.35~2.08) Z=-0.587 0.557 SD(mm) 142.49±27.14 161.29±28.43 t=2.461 0.017 SV(cm3) 459.92±178.33 729.59±290.82 t=4.086 <0.001 PSDR(n·cm-3·mm-1) 536.46(447.82~897.43) 350.29(269.36~529.85) Z=-3.256 0.001 PSVR(n·cm-3·cm-3) 161.74(131.83~282.81) 73.63(55.82~136.00) Z=-3.683 <0.001
下载: 导出CSV
表 3 肝硬化PHG无创指标的Logistic回归分析
Table 3. Logistic regression analysis of non-invasive indexes of PHG in liver cirrhosis
变量 B值 SE Wald P值 OR 95%CI 性别(女=0, 男=1) 0.894 0.647 1.911 0.167 2.445 0.688~8.684 腹水(无=0,有=1) 0.600 0.670 0.802 0.370 1.832 0.490~6.781 Alb -0.101 0.062 2.614 0.106 0.904 0.800~1.022 Child-Pugh分级 0.074 0.819 0.008 0.928 1.077 0.216~5.361 (A=0,B=1,C=2) FIB-4评分 0.247 0.122 4.123 0.042 1.280 1.009~1.625 King评分 -0.016 0.009 2.754 0.097 0.984 0.966~1.003 SD -0.006 0.022 0.077 0.781 0.994 0.953~1.037 SV 0.007 0.003 5.675 0.017 1.007 1.001~1.013 PSDR 0.000 0.001 0.000 0.990 1.000 0.998~1.002 PSVR -0.001 0.002 0.179 0.672 0.999 0.995~1.003
下载: 导出CSV
表 4 肝硬化重度PHG无创指标的Logistic回归分析
Table 4. Logistic regression analysis of non-invasive indexes of severe PHG in liver cirrhosis
变量 B值 SE Wald P值 OR 95%CI PLT 0.017 0.068 0.066 0.797 1.018 0.891~1.162 Alb -0.023 0.077 0.087 0.768 0.977 0.840~1.138 SD 0.054 0.053 1.033 0.310 1.055 0.951~1.171 SV -0.010 0.005 4.073 0.044 0.990 0.980~1.000 PSDR 0.004 0.011 0.125 0.724 1.004 0.983~1.025 PSVR -0.007 0.008 0.751 0.386 0.993 0.978~1.008
下载: 导出CSV
表 5 SV和FIB-4评分诊断PHG,SV诊断重度PHG效能分析
Table 5. Efficiency analysis of SV and FIB-4 in diagnosing PHG, SV in diagnosing severe PHG
变量 AUC 95%CI P值 最佳临界值 敏感度 特异度 约登指数 SV和FIB-4评分诊断PHG SV 0.884 0.829~0.940 <0.001 406.82 0.774 0.870 0.644 FIB-4评分 0.825 0.756~0.894 <0.001 4.05 0.755 0.809 0.563 SV诊断重度PHG 0.782 0.656~0.909 <0.001 714.63 0.593 0.962 0.554
下载: 导出CSV
-
[1] LIU XJ, CHEN MK. Research advances in portal hypertensive gastropathy[J]. Chin J Dig Endosc, 2020, 37(10): 762-765. DOI: 10.3760/cma.j.cn321463-20191014-00688.刘小娇, 陈明锴. 门脉高压性胃病研究进展[J]. 中华消化内镜杂志, 2020, 37(10): 762-765. DOI: 10.3760/cma.j.cn321463-20191014-00688. [2] ROCKEY DC. An update: Portal hypertensive gastropathy and colopathy[J]. Clin Liver Dis, 2019, 23(4): 643-658. DOI: 10.1016/j.cld.2019.07.002. [3] LYLES T, ELLIOTT A, ROCKEY DC. A risk scoring system to predict in-hospital mortality in patients with cirrhosis presenting with upper gastrointestinal bleeding[J]. J Clin Gastroenterol, 2014, 48(8): 712-720. DOI: 10.1097/MCG.0000000000000014. [4] WANG WS, CHEN DF, WEN LZ. Highlights in portal hypertensive gastropathy[J]. J Prac Hepatol, 2019, 22(4): 601-604. DOI: 10.3969/j.issn.1672-5069.2019.04.038.王文生, 陈东风, 文良志. 门脉高压性胃病临床研究进展[J]. 实用肝脏病杂志, 2019, 22(4): 601-604. DOI: 10.3969/j.issn.1672-5069.2019.04.038. [5] AMER IF, EL SHENNAWY EM, EL BATEA H, et al. Accuracy of noninvasive tests in the prediction of portal hypertensive gastropathy in Egyptian patients with cirrhosis[J]. JGH Open, 2021, 5(2): 286-293. DOI: 10.1002/jgh3.12486. [6] EL-KALLA F, MANSOUR L, KOBTAN A, et al. Blood ammonia level correlates with severity of cirrhotic portal hypertensive gastropathy[J]. Gastroenterol Res Pract, 2018, 2018: 9067583. DOI: 10.1155/2018/9067583. [7] NISHINO K, KAWANAKA M, MANABE N, et al. Portal hypertensive gastropathy in liver cirrhosis: Prevalence, natural history, and risk factors[J]. Intern Med, 2022, 61(5): 605-613. DOI: 10.2169/internalmedicine.7943-21. [8] MIN YW, BAE SY, GWAK GY, et al. A clinical predictor of varices and portal hypertensive gastropathy in patients with chronic liver disease[J]. Clin Mol Hepatol, 2012, 18(2): 178-184. DOI: 10.3350/cmh.2012.18.2.178. [9] YU S, CHEN W, JIANG Z. Platelet count/spleen volume ratio has a good predictive value for esophageal varices in patients with hepatitis B liver cirrhosis[J]. PLoS One, 2021, 16(12): e0260774. DOI: 10.1371/journal.pone.0260774. [10] Chinese Society of Hepatology, Chinese Medical Association. Chinese guidelines on the management of liver cirrhosis[J]. J Clin Hepatol, 2019, 35(11): 2408-2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006.中华医学会肝病学分会. 肝硬化诊治指南[J]. 临床肝胆病杂志, 2019, 35(11): 2408-2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006. [11] DE FRANCHIS R. Updating consensus in portal hypertension: report of the Baveno Ⅲ Consensus Workshop on definitions, methodology and therapeutic strategies in portal hypertension[J]. J Hepatol, 2000, 33(5): 846-852. DOI: 10.1016/s0168-8278(00)80320-7. [12] BADRAN DH, KALBOUNEH HM, AL-HADIDI MT, et al. Ultrasonographic assessment of splenic volume and its correlation with body parameters in a Jordanian population[J]. Saudi Med J, 2015, 36(8): 967-972. DOI: 10.15537/smj.2015.8.11809. [13] MOROZOV SV, IZRANOV VA. Methods of ultrasound spleen morphometry[J]. J Ultrasound Med, 2022, 41(9): 2123-2133. DOI: 10.1002/jum.15901. [14] LI Y, WANG ZH, LI PP, et al. 3D visualization technology for measuring the spleen volume of normal Chinese adult[J]. J Hepatobiliary Surg, 2018, 26(5): 340-343. DOI: 10.3969/j.issn.1006-4761.2018.05.007.李曜, 王志恒, 李鹏鹏, 等. 三维可视化技术测定中国正常成人脾脏体积的研究[J]. 肝胆外科杂志, 2018, 26(5): 340-343. DOI: 10.3969/j.issn.1006-4761.2018.05.007. [15] DE FRANCHIS R. Evolving consensus in portal hypertension. Report of the Baveno Ⅳ consensus workshop on methodology of diagnosis and therapy in portal hypertension[J]. J Hepatol, 2005, 43(1): 167-176. DOI: 10.1016/j.jhep.2005.05.009. [16] CHEN SY, LIN QY, HUANG XQ. Studies on diagnosis and pathogenesis of portal hypertensive gastropathy[J]. J Diagn Concepts Pract, 2016, 15(5): 451-454. DOI: 10.16150/j.1671-2870.2016.05.003.陈世耀, 林秋燕, 黄晓铨. 门静脉高压性胃病的诊断及发病机制研究[J]. 诊断学理论与实践, 2016, 15(5): 451-454. DOI: 10.16150/j.1671-2870.2016.05.003. [17] DE FRANCHIS R, BOSCH J, GARCIA-TSAO G, et al. Baveno Ⅶ-Renewing consensus in portal hypertension[J]. J Hepatol, 2022, 76(4): 959-974. DOI: 10.1016/j.jhep.2021.12.022. [18] SALEEM K, BAIG FA, NIDA M, et al. Correlation between severity of portal hypertensive gastropathy and size of oesophageal varices in cirrhotic hepatitis-C patients[J]. J Ayub Med Coll Abbottabad, 2018, 30(1): 54-57. [19] SIMBRUNNER B, BEER A, WÖRAN K, et al. Portal hypertensive gastropathy is associated with iron deficiency anemia[J]. Wien Klin Wochenschr, 2020, 132(1-2): 1-11. DOI: 10.1007/s00508-019-01593-w. [20] SUN DY. Prediction of FIB-4、Lok and King score measurement for esophageal varices in cirrhosis[D]. Hefei: Anhui Medical University, 2021.孙迪一. FIB-4、Lok和King评分对肝硬化食管静脉曲张的预测价值[D]. 合肥: 安徽医科大学, 2021. [21] MANDHWANI R, HANIF FM, UL HAQUE MM, et al. Noninvasive clinical predictors of portal hypertensive gastropathy in patients with liver cirrhosis[J]. J Transl Int Med, 2017, 5(3): 169-173. DOI: 10.1515/jtim-2017-0025. [22] JIANG A, LI ZF. Common causes and treatment strategies of hyperslenism[J/OL]. Chin J Hepat Surg (Electronic Edition), 2018, 7(2): 97-99. DOI: 10.3877/cma.j.issn.2095-3232.2018.02.003 .蒋安, 李宗芳. 脾功能亢进常见原因及治疗策略[J/OL]. 中华肝脏外科手术学电子杂志, 2018, 7(2): 97-99. DOI:10.3877/cma.j.issn.2095-3232.2018.02.003 . -

 本文二维码
本文二维码
计量
- 文章访问数: 249
- HTML全文浏览量: 55
- PDF下载量: 44
- 被引次数: 0

