
 PDF下载 ( 2448 KB)
PDF下载 ( 2448 KB)

远隔缺血预处理联合控制性低中心静脉压在肝切除术中的应用
DOI: 10.3969/j.issn.1001-5256.2023.04.017
伦理学声明:本研究方案于2020年7月6日经由重庆医科大学附属永川医院伦理委员会审批,批号:2020.89。患者及其家属均知情同意并签字。
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突。
作者贡献声明:高苑淞负责收集数据,资料分析,撰写论文;吴悠参与收集数据;杨柳、张娜负责数据统计和资料分析;田春负责课题设计,拟定写作思路,指导撰写文章并最后定稿。
Application of remote ischemic preconditioning combined with controlled low central venous pressure in hepatectomy
-
摘要:
目的 评价远隔缺血预处理(RIPC) 联合控制性低中心静脉压(CLCVP)在肝切除术中的应用效果。 方法 选取2021年5月—2022年4月择期在重庆医科大学附属永川医院行部分肝切除术患者80例,采用随机数表法分成对照组(C组)、CLCVP组(L组)、RIPC组(R组)、RIPC联合CLCVP组(RL组),每组20例。L组接受CLCVP干预,R组接受RIPC干预,RL组同时接受CLCVP和RIPC干预。比较患者术前第1天(D0)、术后第1天(D1)、术后第3天(D3)、术后第5天(D5)、术后第7天(D7) TNFα、ALT、AST、TBil和患者围术期一般情况。正态分布的计量资料组间比较采用单因素方差分析或重复测量方差分析,偏态分布的计量资料组间比较采用Kruskal-Wallis H检验;计数资料组间比较采用χ2检验。 结果 RL组患者手术持续时间(H=14.278, P=0.015)、总输液量(H=24.175, P=0.001)、出血估计量(H=45.625, P<0.001)均低于R组。分组和时间因素对四组患者TNFα、ALT、AST均具有显著交互作用(P值分别为<0.001、0.010、0.012)。RL组患者D1的TNFα均低于L组(P值均<0.001)。RL组患者D1(P=0.008)、D7(P<0.001)ALT水平均低于L组。 结论 RIPC联合CLCVP技术能够有效减少肝切除术患者术中出血量,提供清晰手术视野和缩短手术时间;同时还能通过降低患者TNFα,抑制机体炎症反应,但不能有效减轻CLCVP技术下肝切除术后的肝缺血-再灌注损伤。 Abstract:Objective To investigate the application effect of remote ischemic preconditioning (RIPC) combined with controlled low central venous pressure (CLCVP) in hepatectomy. Methods A total of 80 patients who underwent elective partial hepatectomy in Yougchuan Hospital Affiliated to Chongqing Medical University from May 2021 to April 2022 were enrolled and divided into control group (group C), CLCVP group (group L), RIPC group (group R), and RIPC+CLCVP group (group RL) using a random number table, with 20 patients in each group. The patients in group L received CLCVP, those in group R received RIPC, and those in group RL received both CLCVP and RIPC. The patients were compared in terms of perioperative general status and the levels of tumor necrosis factor-α (TNFα), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin on preoperative day 1(D0), postoperative day 1(D1), postoperative day 3(D3), postoperative day 5(D5), and postoperative day 7(D7). A one-way analysis of variance or a repeated measures analysis of variance was used for comparison of normally distributed continuous data between groups, and the Kruskal-Wallis H test was used for comparison of continuous data with skewed distribution between groups; the chi-square test was used for comparison of categorical data. Results Compared with group R, group RL had a significantly shorter time of operation (H=14.278, P=0.015), a significantly lower total infusion volume (H=24.175, P=0.001), and a significantly lower estimated blood loss (H=45.625, P < 0.001). Group and time factors had significant interaction effects on TNFα, ALT, and AST in the four groups (P < 0.001; P=0.010; P=0.012). Group RL had a significantly lower level of TNFα than group L on D1(P < 0.001) and D3(P < 0.001). Group RL had a significantly lower level of ALT than group L on D1(P=0.008) and D7(P < 0.001). Conclusion For patients undergoing hepatectomy, RIPC combined with CLCVP can effectively reduce intraoperative blood loss, provide a clear surgical field, and shorten the time of operation; meanwhile, it can also inhibit inflammatory response by reducing TNFα, but it cannot effectively alleviate hepatic ischemia-reperfusion injury after hepatectomy under the context of CLCVP. -
Key words:
- Ischemic Preconditioning /
- Central Venous Pressure /
- Reperfusion Injury /
- Hepatectomy
-
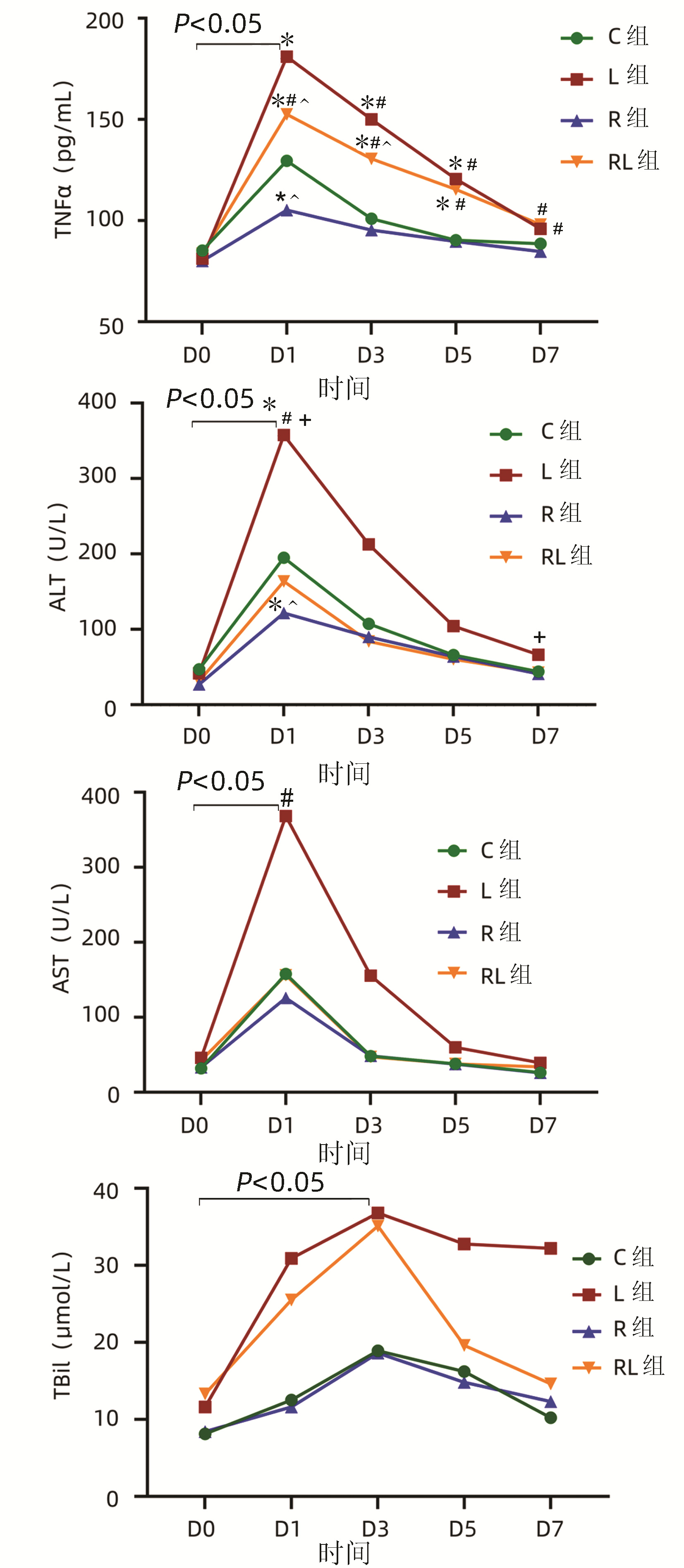
图 1 患者肝功能指标
注:与C组比较,*P<0.01;与R组比较,#P<0.01;与L组比较,∧P<0.01;与RL组比较,+P<0.01。
Figure 1. Liver function variables of patients
表 1 患者基线资料
Table 1. Baseline characteristics of patients
项目 C组(n=20) L组(n=20) R组(n=20) RL组(n=20) 统计值 P值 男/女(例) 12/8 15/5 11/9 13/7 χ2=1.893 0.595 年龄(岁) 61.0(52.0~61.0) 53.5(48.0~62.0) 55.0(53.0~58.8) 55.5(52.0~58.0) H=1.324 0.732 BMI(kg/m2) 23.1±2.1 23.6±2.5 23.7±3.2 23.9±3.7 F=0.284 0.837 ASA分级(Ⅰ/Ⅱ,例) 4/16 6/14 4/16 5/15 χ2=0.829 0.938 既往合并症[例(%)] 高血压 7(35.0) 4(20.0) 6(30.0) 6(30.0) χ2=1.159 0.763 糖尿病 2(10.0) 4(20.0) 3(15.0) 2(10.0) χ2=1.205 0.893 COPD 1(5.0) 0 2(10.0) 1(5.0) χ2=2.097 0.899 肝硬化 14(70.0) 15(75.0) 17(85.0) 13(65.0) χ2=2.260 0.520 D0生化检查 红细胞(×1012/L) 4.4±0.6 4.2±0.3 4.3±0.5 4.4±0.5 F=0.356 0.785 白细胞(×109/L) 6.8±2.5 6.7±2.4 6.4±2.3 6.0±1.4 F=0.617 0.606 中心粒细胞百分比(%) 65.7±10.2 68.4±10.4 66.8±11.6 65.7±10.8 F=0.272 0.845 TNFα(pg/mL) 85.2±10.7 81.2±10.3 80.0±10.9 83.7±11.1 F=0.970 0.412 ALT(U/L) 27.0(18.0~47.0) 29.0(15.3~40.0) 29.0(13.0~39.0) 28.0(13.0~37.5) H=1.407 0.704 AST(U/L) 27.0(19.0~31.0) 34.0(20.8~58.8) 27.0(17.5~34.0) 33.5(20.0~41.0) H=3.227 0.358 TBil(μmol/L) 8.7(5.1~11.5) 11.5(6.9~13.0) 9.3(5.8~10.5) 8.7(6.2~17.7) H=4.264 0.234 白蛋白(g/L) 37.5±5.5 38.6±5.6 40.3±4.1 40.1±3.8 F=1.528 0.214 PT(s) 11.8±1.8 12.3±1.9 11.5±1.1 11.9±1.8 F=0.693 0.559 Cr(μmol/L) 56.0(54.0~63.5) 66.5(45.0~71.0) 65.0(49.0~69.0) 60.0(51.0~63.0) H=2.274 0.436 BUN(mmol/L) 5.1±1.8 5.3±1.6 5.5±1.0 5.1±2.0 F=0.390 0.761  下载: 导出CSV
下载: 导出CSV
表 2 患者麻醉手术一般情况
Table 2. Anesthesia and surgery data of patients
项目 C组(n=20) L组(n=20) R组(n=20) RL组(n=20) 统计值 P值 手术持续时间(min) 260.0(210.0~415.0) 220.0(190.0~300.0)1)2) 285.0(195.0~483.8) 200.0(135.0~295.0)1)2) H=9.053 0.029 肝脏血供阻断时间(min) 62.0(47.0~109.3) 72.0(63.0~97.0) 74.0(49.0~95.0) 67.0(46.8~96.0) H=0.462 0.927 肝脏切除范围[例(%)] χ2=3.211 0.810 肝叶切除 3(15.0) 4(20.0) 5(25.0) 2(10.0) 肝段切除 12(60.0) 14(70.0) 12(60.0) 14(70.0) 不规则肝切除 5(25.0) 2(10.0) 3(15.0) 4(20.0) 术后住院时间(d) 10.4±2.1 11.8±2.2 10.3±1.9 11.4±2.1 F=2.421 0.072 总输液量(L)a 2.8(2.1~3.5) 2.3(2.0~2.5)1)2) 3.0(2.5~3.4) 2.0(2.0~2.5)1)2) H=20.192 <0.001 碳酸氢钠输入量(mL)b 90.0(12.5~145.0) 100.0(90.0~195.0)2) 60.0(0~80.0) 90.0(0~100.0) H=9.952 0.019 术中尿量(mL) 467.5±202.8 465.5±257.9 470.0±120.7 455.5±239.2 F=0.019 0.997 出血估计量(mL) 253.0±48.8 159.0±59.01)2) 285.5±37.5 138.5±31.51)2) F=68.719 <0.001 输血[例(%)] 3(15.0) 0 3(15.0) 1(5.0) χ2=4.080 0.296 升压药[例(%)]c 3(15.0) 6(30.0) 2(10.0) 4(20.0) χ2=2.720 0.491 呋塞米[例(%)] 1(5.0) 5(25.0) 2(10.0) 4(20.0) χ2=3.769 0.335 苏醒延迟[例(%)]d 11(55.0) 9(45.0) 3(15.0) 1)3) 5(25.0) χ2=8.671 0.035 术后并发症情况[例(%)] 2(10.0) 5(25.0) 1(5.0) 3(15.0) χ2=3.381 0.377 新发肺部感染 1(5.0) 2(10.0) 0 2(10.0) 术后切口愈合不良[例(%)] 0 1(5.0) 0 0 术后认知功能障碍 0 1(5.0) 0 0 胸腔积液 0 1(5.0) 1(5.0) 0 麻痹性肠梗阻 1(5.0) 0 0 1(5.0) 注:a, 输液策略为晶胶比1∶1;b, 术中应用5%碳酸氢钠严格控制代谢性酸中毒,使动脉血气分析碱剩余维持在-3~3 mmol/L;c, 术中需使用去甲肾上腺素、麻黄碱、多巴胺等药物维持血压;d, 苏醒延迟即从全身麻醉停药到可被唤醒睁眼或自主睁眼超过90 min。与C组比较,1)P<0.05;与R组比较,2)P<0.05;与L组比较,3)P<0.05。
下载: 导出CSV
-
[1] SUNG H, FERLAY J, SIEGEL RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. DOI: 10.3322/caac.21660. [2] General Office of National Health Commission. Standard for diagnosis and treatment of primary liver cancer(2022 edition)[J]. J Clin Hepatol, 2022, 38(2): 288-303. DOI: 10.3969/j.issn.1001-5256.2022.02.009.国家卫生健康委办公厅. 原发性肝癌诊疗指南(2022年版)[J]. 临床肝胆病杂志, 2022, 38(2): 288-303. DOI: 10.3969/j.issn.1001-5256.2022.02.009. [3] SUN Z, SHAO WW, SONG JH. Progress in diagnosis and treatment of hepatocellular carcinoma with microvascular invasion[J/OL]. Chin J Hepat Surg(Electronic Edition), 2021, 10(3): 235-241. DOI: 10.3877/cma.j.issn.2095-3232.2021.03.002 .孙振, 邵巍伟, 宋京海. 肝细胞癌合并微血管侵犯的诊疗进展[J/OL]. 中华肝脏外科手术学电子杂志, 2021, 10(3): 235-241. DOI:10.3877/cma.j.issn.2095-3232.2021.03.002 .[4] WANG KJ, HUANG ZH, SHI QL, et al. Research progress of precise hepatectomy for hepatocellular carcinoma[J]. China Med Herald, 2021, 18(23): 43-46. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202123010.htm王克净, 黄祖鸿, 石清兰, 等. 肝细胞癌精准肝切除的研究进展[J]. 中国医药导报, 2021, 18(23): 43-46. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202123010.htm [5] RIPAMONTI L, DE CARLIS R, LAUTERIO A, et al. Major hepatectomy for perihilar cholangiocarcinoma in elderly patients: is it reasonable?[J]. Updates Surg, 2022, 74(1): 203-211. DOI: 10.1007/s13304-021-01111-6. [6] HOJO A, NAKAYAMA H, OKAMURA Y, et al. Evaluation of safety-related outcomes of one-segment and more-than-one-segment high-level hepatectomy in hepatocellular carcinoma based on the japanese board certification system[J]. World J Surg, 2022, 46(5): 1141-1150. DOI: 10.1007/s00268-022-06467-3. [7] JUNRUNGSEE S, SUWANNIKOM K, TIYAPRASERTKUL W, et al. Efficacy and safety of infrahepatic inferior vena cava clamping under controlled central venous pressure for reducing blood loss during hepatectomy: A randomized controlled trial[J]. J Hepatobiliary Pancreat Sci, 2021, 28(7): 604-616. DOI: 10.1002/jhbp.969. [8] SHI HZ, XIONG QR, XIA J, et al. Application of controlled low central venous pressure in laparoscopic hepatectomy for patients with primary liver cancer and posthepatitis cirrhosis[J]. Chin J Gen Surg, 2020, 29(1): 27-34. DOI: 10.7659/j.issn.1005-6947.2020.01.004.史惠中, 熊奇如, 夏俊, 等. 控制性低中心静脉压在原发性肝癌伴肝炎后肝硬化患者腹腔镜肝切除中的应用[J]. 中国普通外科杂志, 2020, 29(1): 27-34. DOI: 10.7659/j.issn.1005-6947.2020.01.004. [9] WU G, CHEN M, WANG X, et al. Effect of remote ischemic preconditioning on hepatic ischemia-reperfusion injury in patients undergoing liver resection: a randomized controlled trial[J]. Minerva Anestesiol, 2020, 86(3): 252-260. DOI: 10.23736/S0375-9393.19.13838-2. [10] TEO JY, HO A, BULLUCK H, et al. Effect of remote ischemic preConditioning on liver injury in patients undergoing liver resection: the ERIC-LIVER trial[J]. HPB(Oxford), 2020, 22(9): 1250-1257. DOI: 10.1016/j.hpb.2019.12.002. [11] HIRAO H, NAKAMURA K, KUPIEC-WEGLINSKI JW. Liver ischaemia-reperfusion injury: a new understanding of the role of innate immunity[J]. Nat Rev Gastroenterol Hepatol, 2022, 19(4): 239-256. DOI: 10.1038/s41575-021-00549-8. [12] LIU JD, ZHANG LQ, SHI MZ, et al. Protective effects of modified limb remote ischemic preconditioning on myocardial injury in patients undergoing mitral valve replacement surgery[J]. Chin Circulation J, 2019, 34(3): 272-275. DOI: 10.3969/j.issn.1000-3614.2019.03.012.刘金东, 张连芹, 石梦竹, 等. 改良肢体远端缺血预处理对二尖瓣置换术患者心肌损伤的保护作用[J]. 中国循环杂志, 2019, 34(3): 272-275. DOI: 10.3969/j.issn.1000-3614.2019.03.012. [13] GORJIPOUR F, SAEEDZADEH T, TOLOUEITABAR Y, et al. Remote ischemic preconditioning effects on inflammatory markers and myocardial protection in coronary artery bypass graft surgery[J]. Perfusion, 2022, 37(1): 56-61. DOI: 10.1177/0267659120979293. [14] XIA J, JIA R, QIAN YB, et al. Safety and efficacy of the controlled first hepaticportal blood flow occlusion in hepatectony[J]. Chin J Hepatobiliary Sury, 2021, 27(12): 889-893. DOI: 10.3760/cma.j.cn113884-20210429-00150.夏俊, 贾冉, 钱叶本, 等. 控制性第一肝门阻断法在肝切除手术中的安全性和有效性[J]. 中华肝胆外科杂志, 2021, 27(12): 889-893. DOI: 10.3760/cma.j.cn113884-20210429-00150. [15] LIU XZ, LI MY, REN CN, et al. Specific measures to achieve controlled low central venous pressure during partial hepatectomy[J]. Chin J Hepatobiliary Surg, 2020, 26(6): 469-471. DOI: 10.3760/cma.j.cn113884-20200302-00106.刘秀珍, 李明颖, 任超楠, 等. 大部肝切除术中实现控制性低中心静脉压的具体措施[J]. 中华肝胆外科杂志, 2020, 26(6): 469-471. DOI: 10.3760/cma.j.cn113884-20200302-00106. [16] LIU TS, SHEN QH, ZHOU XY, et al. Application of controlled low central venous pressure during hepatectomy: A systematic review and meta-analysis[J]. J Clin Anesth, 2021, 75: 110467. DOI: 10.1016/j.jclinane.2021.110467. [17] PAN YX, WANG JC, LU XY, et al. Intention to control low central venous pressure reduced blood loss during laparoscopic hepatectomy: A double-blind randomized clinical trial[J]. Surgery, 2020, 167(6): 933-941. DOI: 10.1016/j.surg.2020.02.004. [18] SHI XD, LI BB. Application of controlled low central venous pressure in hepatectomy[J]. J Clin Anesthesiol, 2021, 37(8): 871-874. DOI: 10.12089/jca.2021.08.019.石雪朵, 李冰冰. 控制性低中心静脉压在肝脏切除术中的应用[J]. 临床麻醉学杂志, 2021, 37(8): 871-874. DOI: 10.12089/jca.2021.08.019. [19] LU JC. Application of dobutamine combined with nitroglycerin in ppartial hepatic resection under low central venous pressure[D]. Guangzhou: Guangzhou Medical University, 2020.卢基成. 多巴酚丁胺联合硝酸甘油在控制性低中心静脉压下肝部分切除手术的应用[D]. 广州: 广州医科大学, 2020. [20] ZHANG H, ZHANG T, ZHONG F, et al. Effects of remote ischemic preconditioning on liver injury following hepatectomy: a systematic review and meta-analysis of randomized control trials[J]. Surg Today, 2021, 51(8): 1251-1260. DOI: 10.1007/s00595-020-02205-1. [21] WU J, YU C, ZENG X, et al. The hepatoprotective effect from ischemia-reperfusion injury of remote ischemic preconditioning in the liver related surgery: a meta-analysis[J]. ANZ J Surg, 2022, 92(6): 1332-1337. DOI: 10.1111/ans.17236. [22] MURRY CE, JENNINGS RB, REIMER KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium[J]. Circulation, 1986, 74(5): 1124-1136. DOI: 10.1161/01.cir.74.5.1124. [23] PRZYKLENK K, BAUER B, OVIZE M, et al. Regional ischemic 'preconditioning' protects remote virgin myocardium from subsequent sustained coronary occlusion[J]. Circulation, 1993, 87(3): 893-899. DOI: 10.1161/01.cir.87.3.893. [24] STANKIEWICZ R, GRT M. Direct, remote and combined ischemic conditioning in liver surgery[J]. World J Hepatol, 2021, 13(5): 533-542. DOI: 10.4254/wjh.v13.i5.533. [25] LIU A, FANG H. Ischemic preconditioning on liver ischemia reperfusion injury: How far is the bedside from the bench?[J]. J Invest Surg, 2020, 33(9): 884-885. DOI: 10.1080/08941939.2019.1578443. [26] JAKUBAUSKIENE L, JAKUBAUSKAS M, STIEGLER P, et al. Ischemic preconditioning for liver transplantation: A systematic review and meta-analysis of randomized controlled trials[J]. Visc Med, 2021, 37(5): 329-337. DOI: 10.1159/000516608. [27] KOH WU, KIM J, LEE J, et al. Remote ischemic preconditioning and diazoxide protect from hepatic ischemic reperfusion injury by inhibiting HMGB1-induced TLR4/MyD88/NF-κB signaling[J]. Int J Mol Sci, 2019, 20(23): 5899. DOI: 10.3390/ijms20235899. [28] JULIA S, PETER S, KARL-HEINZ W, et al. Possible role of the HMGB1 and RAGE inflammatory pathway in primary sclerosing cholangitis[J]. Clin Res Hepatol Gastroenterol, 2022, 46(2): 101791. DOI: 10.1016/j.clinre.2021.101791. [29] LIU JH, JIANG W, SHI G, et al. Effect of ischemic preconditioning on liver and kidney function in surgery for large vessels[J]. Chin J Gen Prac, 2019, 17(2): 190-192, 208. DOI: 10.16766/j.cnki.issn.1674-4152.000636.刘建华, 蒋伟, 石光, 等. 大血管手术中应用缺血预处理对肝肾功能的影响[J]. 中华全科医学, 2019, 17(2): 190-192, 208. DOI: 10.16766/j.cnki.issn.1674-4152.000636. [30] SONG IA, JANG ES, OH TK. Validation of dynamic aspartate-to-alanine aminotransferase ratio for predicting liver disease mortality[J]. Hepatol Commun, 2022, 6(4): 740-749. DOI: 10.1002/hep4.1844. [31] KOBAYASHI D, YAMAMOTO K, KIMURA T, et al. Aspartate aminotransferase/alanine aminotransferase ratio and subsequent cancer development[J]. Cancer Med, 2022, 11(3): 798-814. DOI: 10.1002/cam4.4473. [32] LIU X, CAO L, ZHANG T, et al. Effect of remote ischemic preconditioning in patients undergoing hepatectomy with portal triad clamping: A randomized controlled trial[J]. Anesth Analg, 2019, 129(6): 1742-1748. DOI: 10.1213/ANE.0000000000004434. [33] OUYANG S, OUYANG L, LI Y, et al. Bone marrow-derived stem cells for patients with liver cirrhosis: A systematic review and meta-analysis[J]. Turk J Gastroenterol, 2021, 32(10): 896-906. DOI: 10.5152/tjg.2021.19694. -

 本文二维码
本文二维码
图(1) / 表(2)
计量
- 文章访问数: 297
- HTML全文浏览量: 57
- PDF下载量: 31
- 被引次数: 0

