
 PDF下载 ( 2528 KB)
PDF下载 ( 2528 KB)

双向孟德尔随机化分析总胆固醇升高风险与胆石症发生风险的关系
DOI: 10.12449/JCH240322
Association between the risk of increase in total cholesterol and the risk of cholelithiasis: A bidirectional Mendelian randomization study
-
摘要:
目的 运用双向孟德尔随机化评估总胆固醇升高风险与胆石症发生风险之间的关联。 方法 总胆固醇与胆石症相关的单核苷酸多态性数据来自open gwas公共数据库,对基于全基因组相关联研究(GWAS)的所有汇总数据进行二次数据分析,分别选择与总胆固醇或者胆石症密切关联的遗传位点作为暴露或者结局变量,用Egger回归法、加权中位数法、IVW随机效应模型、IVW固定效应模型等方法进行双向孟德尔随机化分析,以OR值评价总胆固醇和胆石症之间的因果关系。 结果 以总胆固醇为暴露、胆石症为结局,去除异质性前总胆固醇-胆石症的总体OR=0.91,95%CI:0.85~0.97;去除异质性后总胆固醇-胆石症的总体OR=0.93,95%CI:0.89~0.97。以胆石症为暴露、总胆固醇为结局,去除异质性前胆石症-总胆固醇的总体OR=0.20,95%CI:0.06~0.65;去除异质性后胆石症-总胆固醇的总体OR=0.28,95%CI:0.10~0.83。基因预测的总胆固醇和胆石症之间存在双向因果关系。 结论 本研究证实了总胆固醇与胆石症之间的双向因果关系,随着遗传上有关能使总胆固醇水平升高的等位基因的增加,发生胆石症的风险降低。反之,随着遗传上有关能使胆石症发病增高的等位基因的增加,总胆固醇水平升高的风险降低。 -
关键词:
- 总胆固醇 /
- 胆石症 /
- 双向孟德尔随机化分析
Abstract:Objective To investigate the association between the risk of increase in total cholesterol (TC) and the risk of cholelithiasis by using bidirectional Mendelian randomization (MR). Methods The open gwas public database was used to obtain the single nucleotide polymorphism data associated with TC and cholelithiasis, and a secondary data analysis was performed for all summary data of genome-wide association studies. The genetic loci closely associated with TC or cholelithiasis were selected as exposure or outcome variables, and the bidirectional MR analysis was performed using the methods such as Egger regression, Weighted median, IVW random effects model, and IVW fixed effects model, with odds ratio (OR) values for evaluating the causal relationship between TC and cholelithiasis. Results With TC as the exposure and cholelithiasis as the outcome, TC-cholelithiasis had an overall OR value of 0.91 (95% confidence interval [CI]: 0.85 — 0.97) before elimination of heterogeneity and 0.93 (95%CI: 0.89 — 0.97) after elimination of heterogeneity. With cholelithiasis as the exposure and TC as the outcome, TC-cholelithiasis had an overall OR value of 0.20 (95%CI: 0.06 — 0.65) before elimination of heterogeneity and 0.28 (95%CI: 0.10 — 0.83) after elimination of heterogeneity. There was a bidirectional causal relationship between genetically predicted TC and cholelithiasis. Conclusion This study confirms the bidirectional causal relationship between TC and cholelithiasis. The risk of cholelithiasis decreases with the increase in alleles associated with the elevation of TC level; on the contrary, the risk of elevated TC level decreases with the increase in alleles associated with the onset of cholelithiasis. -
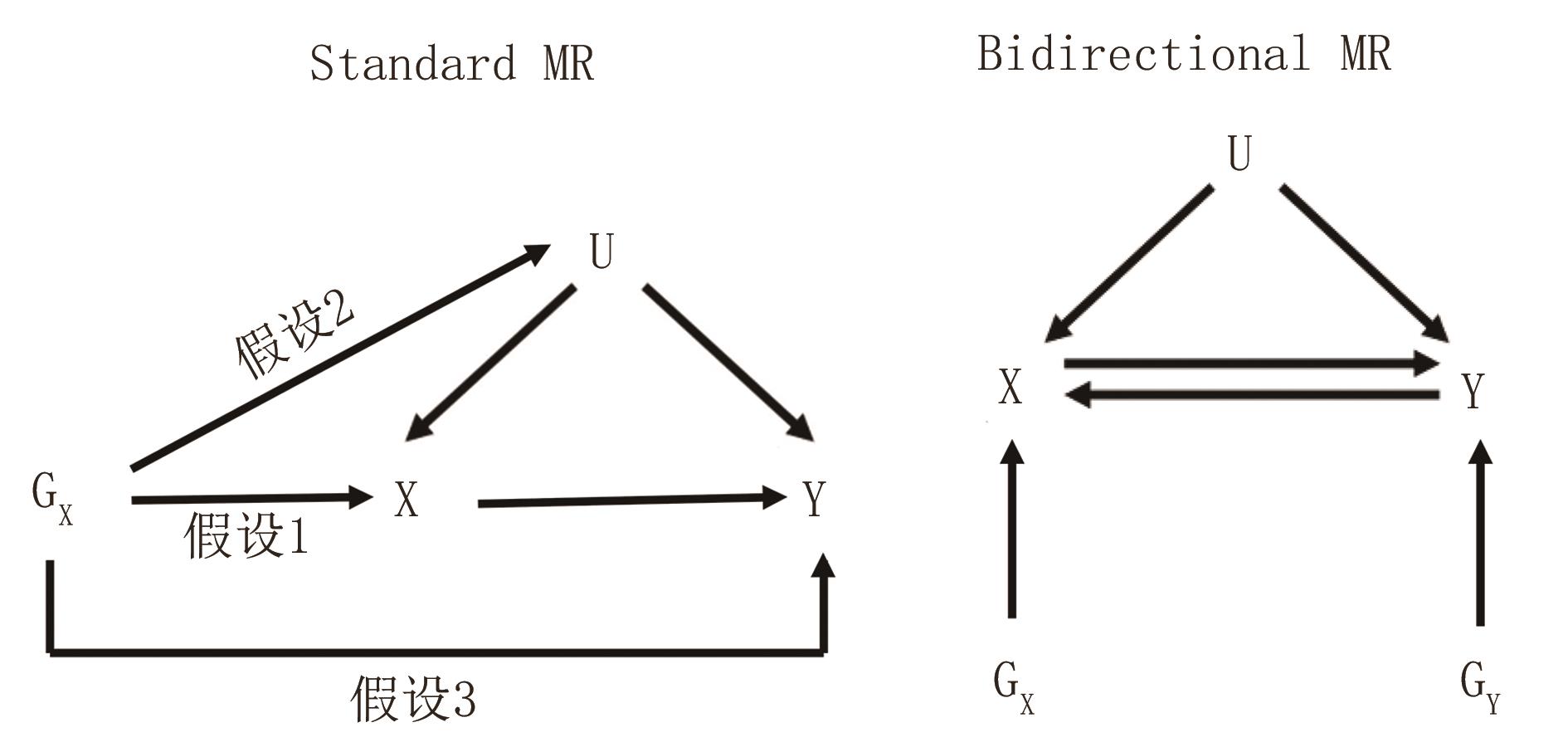
图 1 bidirectional MR的模型图
注: 左侧,普通MR;右侧,bidirectional MR。Gx,工具变量,可用于估计暴露X对结果Y的因果影响。GY,工具变量,可用于估计暴露Y对结果X的因果影响。U:混杂因素。假设1,与暴露显著相关;假设2,与混杂因素不相关;假设3,与结局不相关。
Figure 1. Model diagram of bidirectional Mendelian randomization

图 2 以总胆固醇为暴露、胆石症为结局的MR结果图
注: MR-Egger,Egger回归法;Weighted median,加权中位数法;IVW_mre,随机效应模型;IVW_fe,固定效应模型。nSNP,SNP个数。
Figure 2. MR results of 4 methods with TC as the exposure and cholelithiasis as the outcome

图 3 以胆石症为暴露、总胆固醇为结局的MR结果图
Figure 3. MR results of 4 methods with cholelithiasis as the exposure and TC as the outcome

图 4 以总胆固醇为暴露、胆石症为结局去除异质性后的MR结果图
Figure 4. MR results of 4 methods after removing heterogeneity with TC as the exposure and cholelithiasis as the outcome

图 5 以胆石症为暴露、总胆固醇为结局去除异质性后的MR结果图
Figure 5. MR results of 4 methods after romoving heterogeneity with cholelithiasis as the exposure and TC as the outcome
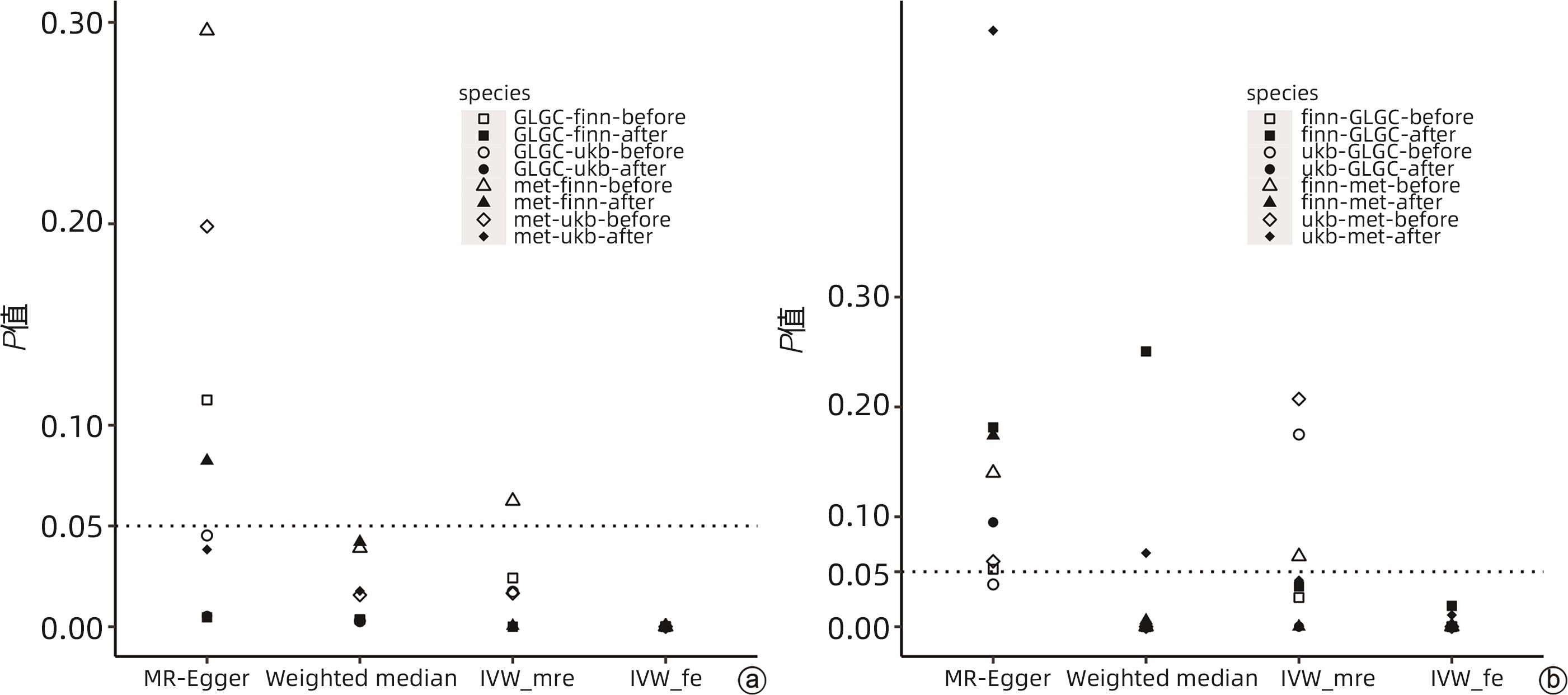
图 6 去除异质性前、后4种MR方法的P值改变
注: a,总胆固醇水平和胆石症之间去除异质性前后P值变化;b,胆石症和总胆固醇之间去除异质性前后P值变化;before,去除异质性前;after,去除异质性后。
Figure 6. The change of P values of MR before and after the removal of heterogeneity
表 1 总胆固醇GWAS数据汇总信息
Table 1. Summary of the GWAS data for total cholesterol
数据来源 种族来源 样本量 SNP个数 公布时间 PMID或数据链接 全球脂质遗传学协会(GLGC) 混合人群 187 365 2 446 982 2013年 24097068 代谢组学研究(met) 欧洲人群 115 078 12 321 875 2020年 Trait: Total cholesterol-IEU OpenGWAS project (mrcieu.ac.uk)  下载: 导出CSV
下载: 导出CSV
表 2 胆石症GWAS数据汇总信息
Table 2. Summary of the GWAS data for cholelithiasis
数据来源 种族来源 样本量 SNP个数 公布时间 PMID或数据链接 英国生物银行(ukb) 欧洲人群 337 199 10 894 596 2017年 Trait: Diagnoses-main ICD10: K80 Cholelithiasis-IEU OpenGWAS project (mrcieu.ac.uk) 芬兰生物银行(finn) 欧洲人群 214 167 16 380 452 2021年 Trait: Cholelithiasis-IEU OpenGWAS project (mrcieu.ac.uk)
下载: 导出CSV
表 3 去除离群SNP前每对暴露-结局数据的工具变量评价及异质性分析结果
Table 3. Results of R²,F and heterogeneity analysis for each pair of expose-outcome data before removing outlier SNP
暴露 结局 总R2 F值 异质性检验 (P值) 多效性检验 (P值) MR-Egger 截距值 I2GX 总胆固醇(GLGC) 胆石症(ukb) 0.019 42.29 1.053×10-110 0.476 91 0.000 97.4% 胆石症(ukb) 总胆固醇(GLGC) 0.001 23.91 2.787×10-79 0.091 80 0.026 97.4% 总胆固醇(met) 胆石症(finn) 0.014 28.57 2.322×10-162 0.919 21 0.000 94.5% 胆石症(finn) 总胆固醇(met) 0.004 27.00 1.132×10-98 0.637 83 0.003 97.0% 总胆固醇(GLGC) 胆石症(finn) 0.019 41.94 0.000 0.777 27 0.003 97.5% 胆石症(finn) 总胆固醇(GLGC) 0.003 32.95 7.713×10-177 0.441 85 0.009 98.1% 总胆固醇(met) 胆石症(ukb) 0.015 29.21 8.971×10-58 0.902 06 0.000 93.5% 胆石症(ukb) 总胆固醇(met) 0.001 23.91 7.428×10-36 0.129 68 0.014 97.2%
下载: 导出CSV
表 4 去除离群SNP后每对暴露-结局数据的工具变量评价及异质性
Table 4. Results of R²,F and heterogeneity analysis for each pair of expose-outcome data after removing outlier SNP
暴露 结局 总R2 F值 异质性检验 (P值) 多效性检验 (P值) MR-Egger截距值 I2GX 总胆固醇(GLGC) 胆石症(ukb) 0.017 0 40.91 0.074 423 0.534 406 0.000 97.6% 胆石症(ukb) 总胆固醇(GLGC) 0.000 2 17.39 0.523 401 0.362 018 0.029 0.0% 总胆固醇(met) 胆石症(finn) 0.009 5 26.85 0.154 922 0.793 729 -0.001 95.5% 胆石症(finn) 总胆固醇(met) 0.001 6 20.29 0.552 098 0.664 215 -0.001 84.7% 总胆固醇(GLGC) 胆石症(finn) 0.015 0 39.74 0.007 047 0.663 828 -0.002 97.7% 胆石症(finn) 总胆固醇(GLGC) 0.000 9 22.32 0.265 042 0.323 317 0.003 63.3% 总胆固醇(met) 胆石症(ukb) 0.014 0 30.11 0.013 513 0.897 168 0.000 93.8% 胆石症(ukb) 总胆固醇(met) 0.000 3 16.22 0.161 575 0.732 752 0.006 0.0%
下载: 导出CSV
-
[1] GERMER CT. Cholelithiasis[J]. Chirurgie(Heidelb), 2022, 93( 6): 533- 534. DOI: 10.1007/s00104-022-01601-2. [2] CHEN L, YANG H, LI H, et al. Insights into modifiable risk factors of cholelithiasis: A Mendelian randomization study[J]. Hepatology, 2022, 75( 4): 785- 796. DOI: 10.1002/hep.32183. [3] ATAMANALP SS, KELES MS, ATAMANALP RS, et al. The effects of serum cholesterol, LDL, and HDL levels on gallstone cholesterol concentration[J]. Pak J Med Sci, 2013, 29( 1): 187- 190. DOI: 10.12669/pjms.291.2798. [4] KAWASHIRI MA, TADA H, NOMURA A, et al. Mendelian randomization: Its impact on cardiovascular disease[J]. J Cardiol, 2018, 72( 4): 307- 313. DOI: 10.1016/j.jjcc.2018.04.007. [5] PAPADIMITRIOU N, DIMOU N, TSILIDIS KK, et al. Physical activity and risks of breast and colorectal cancer: a Mendelian randomisation analysis[J]. Nat Commun, 2020, 11( 1): 597. DOI: 10.1038/s41467-020-14389-8. [6] BOWDEN J, DAVEY SMITH G, HAYCOCK PC, et al. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator[J]. Genet Epidemiol, 2016, 40( 4): 304- 314. DOI: 10.1002/gepi.21965. [7] BOWDEN J, HOLMES MV. Meta-analysis and Mendelian randomization: A review[J]. Res Synth Methods, 2019, 10( 4): 486- 496. DOI: 10.1002/jrsm.1346. [8] SCHERBER PR, ZÚNIGA SE, GLANEMANN M, et al. Gallstone disease-interdisciplinary treatment[J]. Dtsch Med Wochenschr, 2020, 145( 5): 287- 295. DOI: 10.1055/a-0944-8655. [9] LAMMERT F, GURUSAMY K, KO CW, et al. Gallstones[J]. Nat Rev Dis Primers, 2016, 2: 16024. DOI: 10.1038/nrdp.2016.24. [10] LITTLEFIELD A, LENAHAN C. Cholelithiasis: Presentation and management[J]. J Midwifery Womens Health, 2019, 64( 3): 289- 297. DOI: 10.1111/jmwh.12959. [11] BURGESS S, THOMPSON SG. Interpreting findings from Mendelian randomization using the MR-Egger method[J]. Eur J Epidemiol, 2017, 32( 5): 377- 389. DOI: 10.1007/s10654-017-0255-x. [12] BOWDEN J, BURGESS S, DAVEY SG. Response to Hartwig and Davies[J]. Int J Epidemiol, 2016, 45( 5): 1679- 1680. DOI: 10.1093/ije/dyw252. [13] BIRNEY E. Mendelian randomization[J]. Cold Spring Harb Perspect Med, 2022, 12( 4): a041302. DOI: 10.1101/cshperspect.a041302. [14] BURGESS S, DAVEY SMITH G, DAVIES NM, et al. Guidelines for performing Mendelian randomization investigations: update for summer 2023[J]. Wellcome Open Res, 2019, 4: 186. DOI: 10.12688/wellcomeopenres.15555.3. [15] SUN H, WARREN J, YIP J, et al. Factors influencing gallstone formation: a review of the literature[J]. Biomolecules, 2022, 12( 4): 550. DOI: 10.3390/biom12040550. [16] REES J, WOOD AM, BURGESS S. Extending the MR-Egger method for multivariable Mendelian randomization to correct for both measured and unmeasured pleiotropy[J]. Stat Med, 2017, 36( 29): 4705- 4718. DOI: 10.1002/sim.7492. -

 本文二维码
本文二维码
计量
- 文章访问数: 124
- HTML全文浏览量: 51
- PDF下载量: 30
- 被引次数: 0

