
 PDF下载 ( 2079 KB)
PDF下载 ( 2079 KB)

2型糖尿病患者合并非酒精性脂肪性肝病的影响因素分析
DOI: 10.3969/j.issn.1001-5256.2023.05.013
Influencing factors for nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus
-
摘要:
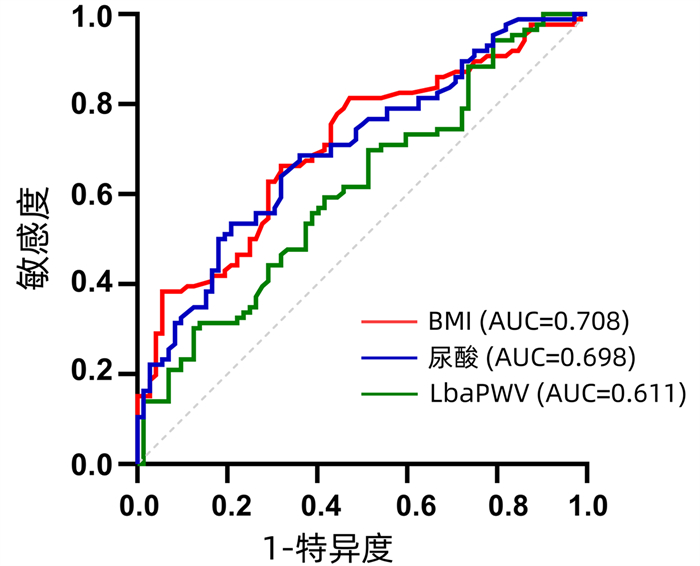
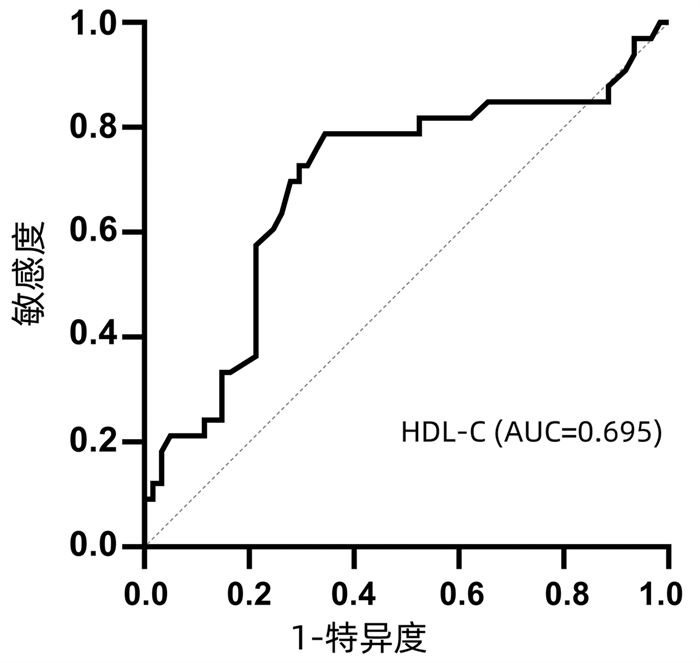
目的 探讨2型糖尿病(T2DM)合并非酒精性脂肪性肝病(NAFLD)患者的相关影响因素。 方法 选取2021年5月—2022年3月上海市宝山区中西医结合医院中纳入国家标准化代谢性疾病管理中心的252例T2DM患者,根据患者的脂肪肝情况,分为单纯T2DM组(n=105)和T2DM合并NAFLD组(n=147)。分析患者一般资料,包括性别、年龄、血压、身高、体质量、颈围、甘油三酯(TG)、总胆固醇、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇、空腹血糖、糖化血红蛋白、超敏C反应蛋白、晨尿白蛋白/肌酐、促甲状腺激素、尿酸、肝内脂肪沉积情况、颈动脉内膜中层厚度以及踝臂脉搏波等。正态分布的计量资料两组间比较采用成组t检验;非正态分布的计量资料两组间比较采用Mann-Whitney U检验。计数资料组间比较采用χ2检验。多因素Logistic回归分析T2DM合并NAFLD的相关危险因素,应用受试者工作特征曲线(ROC曲线)评估相关影响因素的预测价值。 结果 按年龄分层统计分析发现,<50岁T2DM合并NAFLD患者的BMI、内脏脂肪、TG、肱踝脉搏波传导速度、晨尿白蛋白/肌酐、尿酸水平均显著高于单纯T2DM患者(P值均<0.05),血清HDL-C水平显著低于单纯T2DM患者(P<0.05);≥50岁T2DM合并NAFLD患者的血压、BMI、内脏脂肪、TG、肱踝脉搏波传导速度、晨尿白蛋白/肌酐、尿酸水平显著高于单纯T2DM患者(P值均<0.05),血清HDL-C水平显著低于单纯T2DM患者(P<0.05)。多因素Logistic回归分析结果显示,BMI(OR=1.408,95%CI:1.136~1.746,P=0.002)、HDL-C(OR=0.031,95%CI:0.001~0.647,P=0.025)、左肱踝脉搏波传导速度(OR=1.003,95%CI:1.001~1.006,P=0.003)、尿酸(OR=1.011,95%CI:1.005~1.016,P<0.001)是T2DM合并NAFLD的独立影响因素。ROC曲线结果显示,HDL-C、BMI、左肱踝脉搏波传导速度、尿酸评估T2DM合并NAFLD的曲线下面积分别为0.695(95%CI:0.574~0.812)、0.708(95%CI:0.628~0.788)、0.611(95%CI:0.523~0.698)、0.698(95%CI:0.617~0.779)。 结论 低水平HDL-C、BMI、左肱踝脉搏波传导速度及尿酸对T2DM患者NAFLD发生具有预测价值。 Abstract:Objective To investigate related influencing factors in patients with type 2 diabetes mellitus (T2DM) and nonalcoholic fatty liver disease (NAFLD). Methods A total of 252 patients with T2DM who were treated in Shanghai Baoshan Hospital of Integrated Traditional Chinese and Western Medicine from May 2021 to March 2022 were enrolled as subjects, and these patients were also included in Metabolic Management Center of China. According to the presence or absence of fatty liver disease, the patients were divided into simple T2DM group (n=105) and T2DM+NAFLD group (n=147). Related general data were analyzed, including sex, age, blood pressure, body height, body weight, neck circumference, triglyceride (TG), total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol, fasting blood glucose, glycosylated hemoglobin, high-sensitivity C-reactive protein, albumin/creatinine ratio in morning urine, thyroid stimulating hormone, uric acid, intrahepatic fat deposition, carotid intima-media thickness, and brachial-ankle pulse wave velocity. The group t-test was used for comparison of normally distributed continuous data between two groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test was used for comparison of categorical data between groups. A multivariate logistic regression analysis was used to investigate the risk factors for T2DM with NAFLD, and the receiver operating characteristic (ROC) curve was used to assess the predictive value of related influencing factors. Results The age-stratified analysis showed that in the < 50 years age group, compared with the patients with T2DM alone, the patients with T2DM and NAFLD had significantly higher levels of body mass index (BMI), visceral fat, TG, brachial-ankle pulse wave velocity, albumin/creatinine ratio in morning urine, and uric acid (P < 0.05); in the ≥50 years age group, compared with the patients with T2DM alone, the patients with T2DM and NAFLD had significantly higher levels of blood pressure, BMI, visceral fat, TG, brachial-ankle pulse wave velocity, albumin/creatinine ratio in morning urine, and uric acid (P < 0.05) and a significantly lower level of serum HDL-C (P < 0.05). The multivariate logistic regression analysis showed that BMI (odds ratio [OR]=1.408, 95% confidence interval [CI]: 1.136-1.746, P=0.002), HDL-C (OR=0.031, 95% CI: 0.001-0.647, P=0.025), left brachial-ankle pulse wave velocity (OR=1.003, 95% CI: 1.001-1.006, P=0.003), and uric acid (OR=1.011, 95% CI: 1.005-1.016, P < 0.001) were independent influencing factors for T2DM with NAFLD. The ROC curve analysis showed that HDL-C, BMI, left brachial-ankle pulse wave velocity, and uric acid had an area under the ROC curve of 0.695 (95% CI: 0.574-0.812), 0.708 (95% CI: 0.628-0.788), 0.611 (95% CI: 0.523-0.698), and 0.698 (95% CI: 0.617-0.779), respectively, in evaluating T2DM with NAFLD. Conclusion Low levels of HDL-C, BMI, left brachial-ankle pulse wave velocity, and uric acid have a certain value in predicting NAFLD in patients with T2DM. -
表 1 50岁以下患者一般资料比较
Table 1. Baseline data and univariate analysis of patients under 50 years old
指标 总体(n=94) 单纯T2DM组(n=33) T2DM合并NAFLD组(n=61) 统计值 P值 男/女(例) 65/29 21/12 44/17 χ2= 0.724 0.395 年龄(岁) 42.00(36.50~45.00) 42.00(34.50~45.00) 42.00(37.00~45.75) Z=-0.540 0.589 舒张压(mmHg) 84.68±10.12 83.18±12.16 85.62±8.90 t=-1.112 0.269 收缩压(mmHg) 132.15±17.60 129.45±21.69 133.67±14.76 t=-0.999 0.323 BMI(kg/m2) 27.20(23.60~30.90) 24.00(22.65~27.20) 28.70(26.18~31.93) Z=-3.672 <0.001 内脏脂肪(cm2) 99.89±43.50 75.82±38.67 112.93±40.16 t=-4.332 <0.001 FBG(mmol/L) 7.80(6.45~10.00) 7.30(6.20~9.00) 8.35(6.32~10.35) Z=-1.383 0.167 HbA1c(%) 9.46±2.11 8.99±2.21 9.76±2.02 t=-1.701 0.092 TG(mmol/L) 1.61(1.12~2.32) 1.25(0.79~1.72) 1.73(1.34~2.96) Z=-3.680 <0.001 TC(mmol/L) 4.80±1.01 4.72±0.87 4.84±1.16 t=-0.528 0.599 HDL-C(mmol/L) 0.97(0.80~1.12) 1.10(0.98~1.17) 0.93(0.79~1.06) Z=-3.082 0.002 LDL-C(mmol/L) 3.28±0.83 3.24±0.82 3.31±0.83 t=-0.322 0.748 hsCRP(mg/L) 1.38(0.61~4.79) 1.18(0.57~3.01) 1.95(0.62~5.67) Z=-1.153 0.249 右颈IMT(μm) 70.0(60.5~80.0) 70.0(60.0~80.0) 70.5(64.0~80.0) Z=-1.442 0.149 左颈IMT(μm) 70.0(60.0~80.0) 70.0(60.0~80.0) 74.0(67.5~80.0) Z=-1.880 0.060 左踝臂指数 1.04±0.10 1.06±0.08 1.03±0.11 t=1.764 0.081 右踝臂指数 1.07±0.11 1.09±0.10 1.06±0.10 t=1.681 0.096 LbaPWV(cm/s) 1 384.19±205.61 1 297.97±234.77 1 429.79±171.15 t=-3.118 0.006 RbaPWV(cm/s) 1 382.29±195.47 1 315.03±237.12 1 418.14±157.54 t=-2.244 0.029 晨尿白蛋白/肌酐(mg/g) 30.00(22.00~45.00) 26.00(20.00~36.00) 34.50(24.25~48.75) Z=-2.358 0.018 TSH(μIU/mL) 1.45(1.01~2.42) 1.44(0.99~2.44) 1.47(1.02~2.34) Z=-0.091 0.927 颈围(cm) 40.00(37.50~44.00) 39.00(35.75~42.50) 40.00(39.00~44.75) Z=-1.899 0.058 尿酸(μmol/L) 355.68±96.92 327.61±99.98 370.41±91.82 t=-2.091 0.039 注:LbaPWV,左肱踝脉搏波传导速度;RbaPWV,右肱踝脉搏波传导速度。  下载: 导出CSV
下载: 导出CSV
表 2 50岁以上患者一般资料比较
Table 2. Baseline data and univariate analysis of patients over 50 years old
指标 总体(n=158) 单纯T2DM组(n=72) T2DM合并NAFLD组(n=86) 统计值 P值 男/女(例) 100/58 49/23 51/35 χ2=1.292 0.256 年龄(岁) 59.00(56.00~64.00) 60.00(56.00~66.00) 58.00(54.00~63.25) Z=-1.205 0.228 舒张压(mmHg) 79.93±10.41 77.11±9.07 82.22±10.89 t=-3.170 0.002 收缩压(mmHg) 133.88±20.32 129.10±17.40 137.86±21.66 t=-2.770 0.006 BMI(kg/m2) 25.3(23.3~27.9) 23.8(22.6~26.7) 26.5(24.3~28.8) Z=-4.494 <0.001 内脏脂肪(cm2) 87.0(67.5~113.5) 75.0(57.0~105.0) 97.0(76.0~125.0) Z=-3.857 <0.001 FBG(mmol/L) 6.9(5.8~8.9) 6.6(5.8~8.4) 7.3(5.8~9.3) Z=-1.589 0.112 HbA1c(%) 8.60(7.25~9.80) 7.90(7.10~9.80) 8.75(7.58~9.73) Z=-1.235 0.217 TG(mmol/L) 1.40(1.01~2.05) 1.27(0.94~1.81) 1.55(1.14~2.31) Z=-2.849 0.004 TC(mmol/L) 4.56(4.02~5.54) 4.61(3.93~5.32) 4.48(4.09~5.61) Z=-0.592 0.554 HDL-C(mmol/L) 1.08(0.88~1.27) 1.13(0.92~1.34) 1.06(0.85~1.20) Z=-2.250 0.024 LDL-C(mmol/L) 3.10±0.88 3.04±0.90 3.15±0.90 t=0.744 0.458 hsCRP(mg/L) 2.10(0.65~3.59) 1.53(0.50~3.24) 2.34(0.89~3.83) Z=-1.309 0.191 右颈IMT(μm) 80(70~80) 80(63~80) 80(70~80) Z=-0.719 0.472 左颈IMT(μm) 80(70~81) 80(66~80) 80(70~81) Z=-1.094 0.274 左踝臂指数 1.10(1.02~1.16) 1.12(1.02~1.18) 1.08(1.01~1.15) Z=-1.425 0.154 右踝臂指数 1.12(1.04~1.20) 1.15(1.04~1.21) 1.11(1.03~1.19) Z=-1.471 0.141 LbaPWV(cm/s) 1 600.0(1 416.0~1 798.5) 1 547.0(1 343.0~1 731.0) 1 652.5(1 422.0~1 872.0) Z=-2.390 0.017 RbaPWV(cm/s) 1 554.0(1 398.5~1 777.0) 1 508.0(1 360.0~1 716.0) 1 639.5(1 402.8~1 851.8) Z=-2.350 0.019 晨尿白蛋白/肌酐(mg/g) 30.00(20.00~47.00) 24.00(17.00~34.00) 35.50(23.00~55.75) Z=-3.124 0.002 TSH(μIU/mL) 1.69(1.16~2.38) 1.71(1.21~2.26) 1.64(1.11~2.49) Z=-0.187 0.852 颈围(cm) 38.00(35.75~41.00) 38.00(35.00~40.00) 39.00(36.00~42.00) Z=-1.697 0.090 尿酸(μmol/L) 307.0(262.0~374.5) 288.0(246.0~329.0) 342.0(289.0~403.5) Z=-4.286 <0.001
下载: 导出CSV
表 3 50岁以下患者组多因素Logistic回归分析
Table 3. Multivariate Logistic regression analysis of patients under 50 years old
指标 OR 95%CI P值 BMI(kg/m2) 1.131 0.912~1.403 0.263 内脏脂肪(cm2) 1.020 0.994~1.047 0.126 TG(mmol/L) 1.231 0.612~2.474 0.560 HDL-C(mmol/L) 0.031 0.001~0.647 0.025 LbaPWV(cm/s) 1.004 0.999~1.009 0.082 RbaPWV(cm/s) 1.002 0.997~1.007 0.488 晨尿白蛋白/肌酐(mg/g) 0.999 0.994~1.004 0.775 尿酸(μmol/L) 0.999 0.992~1.006 0.766
下载: 导出CSV
表 4 50岁以上患者组多因素Logistic回归分析
Table 4. Multivariate Logistic regression analysis of patients over 50 years old
指标 OR 95%CI P值 舒张压(mmHg) 1.049 0.996~1.106 0.072 收缩压(mmHg) 0.971 0.941~1.002 0.064 BMI(kg/m2) 1.408 1.136~1.746 0.002 内脏脂肪(cm2) 0.993 0.975~1.011 0.454 TG(mmol/L) 0.976 0.760~1.255 0.852 HDL-C(mmol/L) 0.582 0.117~2.889 0.508 LbaPWV(cm/s) 1.003 1.001~1.006 0.003 RbaPWV(cm/s) 1.000 0.999~1.000 0.187 晨尿白蛋白/肌酐(mg/g) 0.999 0.996~1.001 0.257 尿酸(μmol/L) 1.011 1.005~1.016 <0.001
下载: 导出CSV
-
[1] International Diabetes Federation. IDF Diabetes Atlas 10th edition[EB/OL]. (2021-11-08)[2022-08-16]. https://diabetesatlas.org/data/en/world/ .[2] Chinese Society of Endocrinology, Chinese Medical Association. Consensus for diagnosis and treatment of nonalcoholic fatty liver diseases and metabolic disorders (2nd Edition)[J]. J Clin Hepatol, 2018, 34(10): 2103-2108. DOI: 10.3969/j.issn.1001-5256.2018.10.010.中华医学会内分泌学分会. 非酒精性脂肪性肝病与相关代谢紊乱诊疗共识(第二版)[J]. 临床肝胆病杂志, 2018, 34(10): 2103-2108. DOI: 10.3969/j.issn.1001-5256.2018.10.010. [3] ZHOU Q, WANG Y, WANG J, et al. Prevalence and risk factor analysis for the nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus[J]. Medicine (Baltimore), 2021, 100(10): e24940. DOI: 10.1097/MD.0000000000024940. [4] SONG T, JIA Y, LI Z, et al. Effects of liraglutide on nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus: a systematic review and meta-analysis[J]. Diabetes Ther, 2021, 12(6): 1735-1749. DOI: 10.1007/s13300-021-01072-4. [5] YOUNOSSI ZM, GOLABI P, de AVILA L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis[J]. J Hepatol, 2019, 71(4): 793-801. DOI: 10.1016/j.jhep.2019.06.021. [6] Chinese Society of Diabetes, Chinese Medical Association. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition)[J]. Chin J Diabetes Mellitus, 2018, 10(1): 4-67. DOI: 10.3760/cma.j.issn.1674-5809.2018.01.003.中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2017年版)[J]. 中华糖尿病杂志, 2018, 10(1): 4-67. DOI: 10.3760/cma.j.issn.1674-5809.2018.01.003. [7] National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology, Chinese Medical Association; Fatty Liver Expert Committee, Chinese Medical Doctor Association. Guidelines of prevention and treatment for nonalcoholic fatty liver disease: A 2018 update[J]. J Clin Hepatol, 2018, 34(5): 947-957. DOI: 10.3969/j.issn.1001-5256.2018.05.007.中华医学会肝病学分会脂肪肝和酒精性肝病学组, 中国医师协会脂肪性肝病专家委员会. 非酒精性脂肪性肝病防治指南(2018年更新版)[J]. 临床肝胆病杂志, 2018, 34(5): 947-957. DOI: 10.3969/j.issn.1001-5256.2018.05.007. [8] WANG L, PENG W, ZHAO Z, et al. Prevalence and treatment of diabetes in China, 2013-2018[J]. JAMA, 2021, 326(24): 2498-2506. DOI: 10.1001/jama.2021.22208. [9] NAN Y, AN J, BAO J, et al. The Chinese Society of Hepatology position statement on the redefinition of fatty liver disease[J]. J Hepatol, 2021, 75(2): 454-461. DOI: 10.1016/j.jhep.2021.05.003. [10] BUZZETTI E, PINZANI M, TSOCHATZIS EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD)[J]. Metabolism, 2016, 65(8): 1038-1048. DOI: 10.1016/j.metabol.2015.12.012. [11] TARGHER G, COREY KE, BYRNE CD, et al. The complex link between NAFLD and type 2 diabetes mellitus-mechanisms and treatments[J]. Nat Rev Gastroenterol Hepatol, 2021, 18(9): 599-612. DOI: 10.1038/s41575-021-00448-y. [12] ZHANG M, CHEN L, QU MD, et al. Analysis of the risk factors for NAFLD in patients with T2DM[J]. Parenter Enteral Nutr, 2019, 26(5): 271-275. DOI: 10.16151/j.1007-810x.2019.05.004.张敏, 陈璐, 瞿美娣, 等. 2型糖尿病病人合并非酒精性脂肪性肝病的危险因素分析[J]. 肠外与肠内营养, 2019, 26(5): 271-275. DOI: 10.16151/j.1007-810x.2019.05.004. [13] MA HL, QUAN L, JIANG S. Analysis of clinical characteristics and risk factors in patients with nonal-coholic fatty liver disease complicated with type 2 diabetes mellitus[J]. China Med Herald, 2022, 19(21): 70-73, 82. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202221016.htm马海林, 权莉, 蒋升. 非酒精性脂肪性肝病合并2型糖尿病患者的临床特征及危险因素分析[J]. 中国医药导报, 2022, 19(21): 70-73, 82. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202221016.htm [14] MANGLA N, AJMERA VH, CAUSSY C, et al. Liver stiffness severity is associated with increased cardiovascular risk in patients with type 2 diabetes[J]. Clin Gastroenterol Hepatol, 2020, 18(3): 744-746. DOI: 10.1016/j.cgh.2019.05.003. [15] MUZICA CM, SFARTI C, TRIFAN A, et al. Nonalcoholic fatty liver disease and type 2 diabetes mellitus: a bidirectional relationship[J]. Can J Gastroenterol Hepatol, 2020, 2020: 6638306. DOI: 10.1155/2020/6638306. [16] ALEMANY-PAGÈS M, MOURA-RAMOS M, ARAÚJO S, et al. Insights from qualitative research on NAFLD awareness with a cohort of T2DM patients: time to go public with insulin resistance?[J]. BMC Public Health, 2020, 20(1): 1142. DOI: 10.1186/s12889-020-09249-5. [17] VUSIRIKALA A, THOMAS T, BHALA N, et al. Impact of obesity and metabolic health status in the development of non-alcoholic fatty liver disease (NAFLD): A United Kingdom population-based cohort study using the health improvement network (THIN)[J]. BMC Endocr Disord, 2020, 20(1): 96. DOI: 10.1186/s12902-020-00582-9. [18] AMPUERO J, RANCHAL I, GALLEGO-DURÁN R, et al. Oxidized low-density lipoprotein antibodies/high-density lipoprotein cholesterol ratio is linked to advanced non-alcoholic fatty liver disease lean patients[J]. J Gastroenterol Hepatol, 2016, 31(9): 1611-1618. DOI: 10.1111/jgh.13335. [19] ALONSO-DOMÍNGUEZ R, SÁNCHEZ-AGUADERO N, PATINO-ALONSO MC, et al. Association between measurements of arterial stiffness and target organ damage in a general Spanish population[J]. Ann Med, 2021, 53(1): 345-356. DOI: 10.1080/07853890.2021.1881812. [20] CAUSSY C, AUBIN A, LOOMBA R. The relationship between type 2 diabetes, NAFLD, and cardiovascular risk[J]. Curr Diab Rep, 2021, 21(5): 15. DOI: 10.1007/s11892-021-01383-7. [21] American Diabetes Association Professional Practice Committee. Addendum. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022;45(Suppl. 1): S144-S174[J]. Diabetes Care, 2022, 45(9): 2178-2181. DOI: 10.2337/dc22-ad08 .[22] CUI Y, LIU J, SHI H, et al. Serum uric acid is positively associated with the prevalence of nonalcoholic fatty liver in non-obese type 2 diabetes patients in a Chinese population[J]. J Diabetes Complications, 2021, 35(5): 107874. DOI: 10.1016/j.jdiacomp.2021.107874. [23] HE J, YE J, SUN Y, et al. The additive values of the classification of higher serum uric acid levels as a diagnostic criteria for metabolic-associated fatty liver disease[J]. Nutrients, 2022, 14(17): 3587. DOI: 10.3390/nu14173587. -

 本文二维码
本文二维码
计量
- 文章访问数: 540
- HTML全文浏览量: 200
- PDF下载量: 79
- 被引次数: 0

