
 PDF下载 ( 2586 KB)
PDF下载 ( 2586 KB)

血浆致动脉粥样硬化指数预测2型糖尿病发生代谢相关脂肪性肝病的价值分析
DOI: 10.3969/j.issn.1001-5256.2023.06.012
Value of atherogenic index of plasma in predicting metabolic associated fatty liver disease in patients with type 2 diabetes mellitus
-
摘要:
目的 探讨血浆致动脉粥样硬化指数(AIP)与2型糖尿病(T2DM)合并代谢相关脂肪性肝病(MAFLD)的关系。 方法 2021年9月—2022年9月于郑州大学第一附属医院内分泌科住院治疗的T2DM患者375例,根据是否合并MAFLD分为T2DM合并MAFLD组(T2DM+MAFLD组,n=245)和T2DM组(T2DM组,n=130)。记录患者的临床资料,并计算AIP。根据AIP四分位数将受试者分为四组:Q1组,AIP≤0.20;Q2组: 0.20<AIP≤0.24;Q3组:0.24<AIP≤0.48;Q4组: AIP>0.48。正态分布的计量资料组间比较采用成组t检验;非正态分布计量资料组间比较采用Wilcoxon秩和检验;计数资料趋势性分析采用趋势χ2检验。采用多因素Logistic回归探讨AIP对MAFLD的影响;采用受试者工作特征曲线(ROC曲线)评估AIP、BMI、ALT等指标对T2DM合并MAFLD的预测价值。 结果 与T2DM组相比,T2DM+MAFLD组BMI、收缩压、尿酸、空腹血糖、糖化血红蛋白、ALT、AST、GGT、ALP、甘油三酯、低密度脂蛋白、AIP水平均明显升高,而高密度脂蛋白水平降低(P值均<0.05)。趋势χ2检验显示T2DM患者MAFLD的患病率随AIP水平的升高而呈增加趋势(χ趋势2=20.338,P<0.05)。多因素Logistic回归分析显示与Q1组相比,Q4组(OR=2.396,95%CI:1.018~5.640)发生MAFLD的风险增加(P=0.045)。ROC曲线分析结果显示,AIP联合ALT、BMI作为诊断模型有最佳的诊断效能(AUC=0.816),最佳临界值为0.670,灵敏度为70.2%,特异度78.5%。 结论 AIP是T2DM合并MAFLD的独立危险因素,其中AIP联合BMI、ALT对T2DM合并MAFLD有较好的预测价值。 -
关键词:
- 血浆致动脉粥样硬化指数 /
- 糖尿病, 2型 /
- 非酒精性脂肪性肝病
Abstract:Objective To investigate the association between atherogenic index of plasma (AIP) and metabolic associated fatty liver (MAFLD) in type 2 diabetes mellitus (T2DM). Methods A total of 375 patients with T2DM who were hospitalized and treated in Department of Endocrinology, The First Affiliated Hospital of Zhengzhou University, from September 2021 to September 2022 were enrolled, and according to the presence or absence of MAFLD, they were divided into T2DM+MAFLD group with 245 patients and T2DM group with 130 patients. Related clinical data were recorded, and AIP was calculated. According to the quartiles of AIP, the patients were divided into Q1 group (AIP≤0.20), Q2 group (0.20 < AIP≤0.24), Q3 group (0.24 < AIP≤0.48), and Q4 group (AIP > 0.48). The independent-samples t test was used for comparison of normally distributed continuous data between groups, and the Wilcoxon rank-sum test was used for comparison of non-normally distributed continuous data between groups; the trend chi-square test was used for the trend analysis of categorical data. The multivariate logistic regression analysis was used to investigate the effect of AIP on MAFLD, and the receiver operating characteristic (ROC) curve and the area under the ROC curve (AUC) were used to assess the value of the indicators such as AIP, body mass index (BMI), and alanine aminotransferase (ALT) in predicting T2DM with MAFLD. Results Compared with the T2DM group, the T2DM+MAFLD group had significant increases in BMI, systolic pressure, uric acid, fasting blood glucose, glycosylated hemoglobin, ALT, aspartate aminotransferase, gamma-glutamyl transpeptidase, alkaline phosphatase, triglyceride, low-density lipoprotein, and AIP and a significant reduction in high-density lipoprotein (all P < 0.05). The trend chi-square test showed that the prevalence rate of MAFLD in T2DM patients tended to increase with the increase in AIP level (χtrend2=20.338, P < 0.05). The multivariate logistic regression analysis showed that compared with the Q1 group, the Q4 group had a significant increase in the risk of MAFLD (odds ratio =2.396, 95% confidence interval: 1.018-5.640, P=0.045). The ROC curve analysis showed that the diagnostic model of AIP combined with BMI and ALT had the best diagnostic performance (AUC=0.816), with a sensitivity of 70.2% and a specificity of 78.5% at the optimal cut-off value of 0.670. Conclusion AIP is an independent risk factor for MAFLD in T2DM patients, and AIP combined with BMI and ALT has a good predictive value for T2DM with MAFLD. -
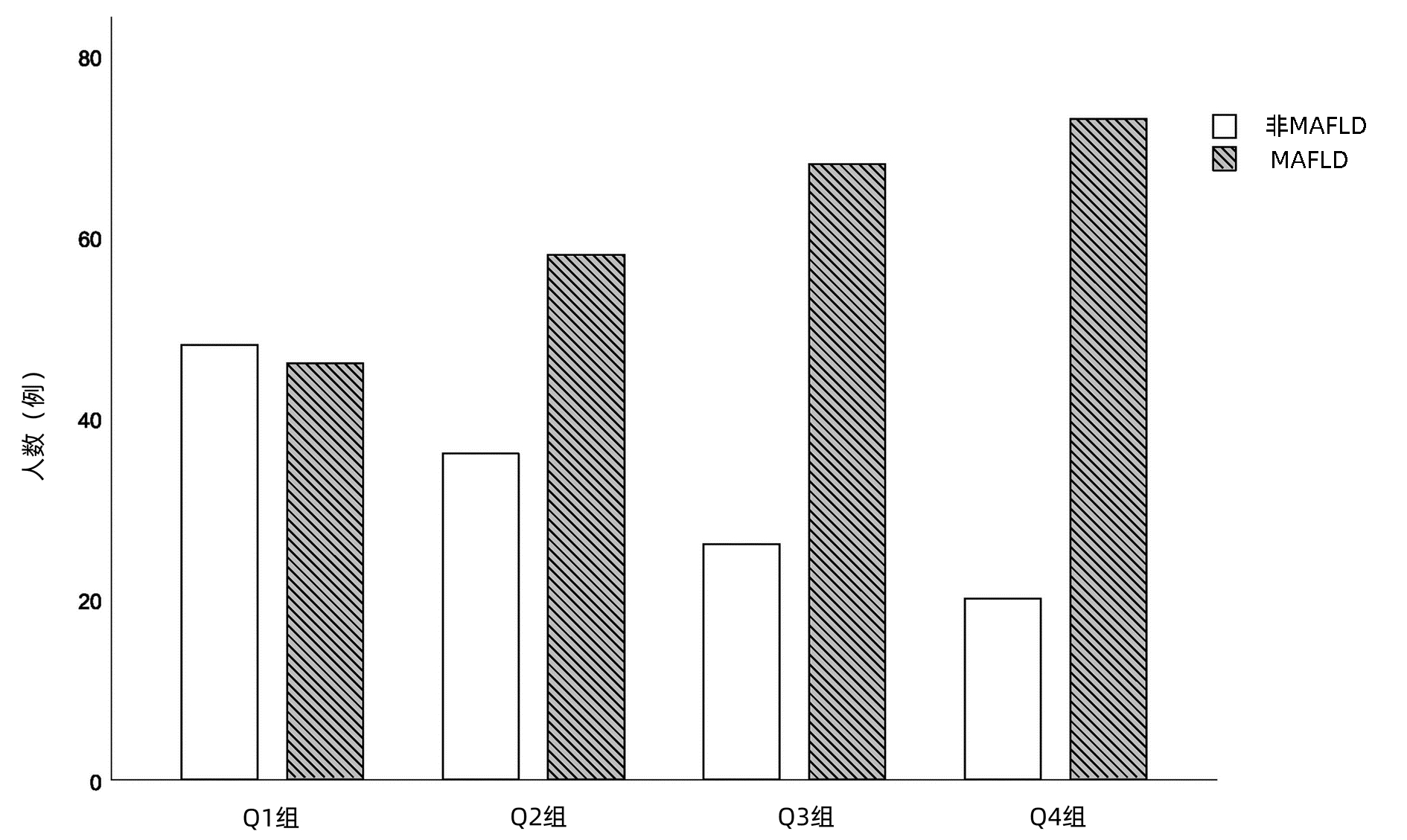
图 1 AIP 4组间T2DM合并MAFLD患病率的比较
Figure 1. Relationship between AIP quartile and the prevalence of fatty liver disease

图 2 AIP、BMI、ALT及三者联合预测MAFLD的ROC曲线
Figure 2. ROC curves of AIP, BMI, ALT and their combination to predict MAFLD
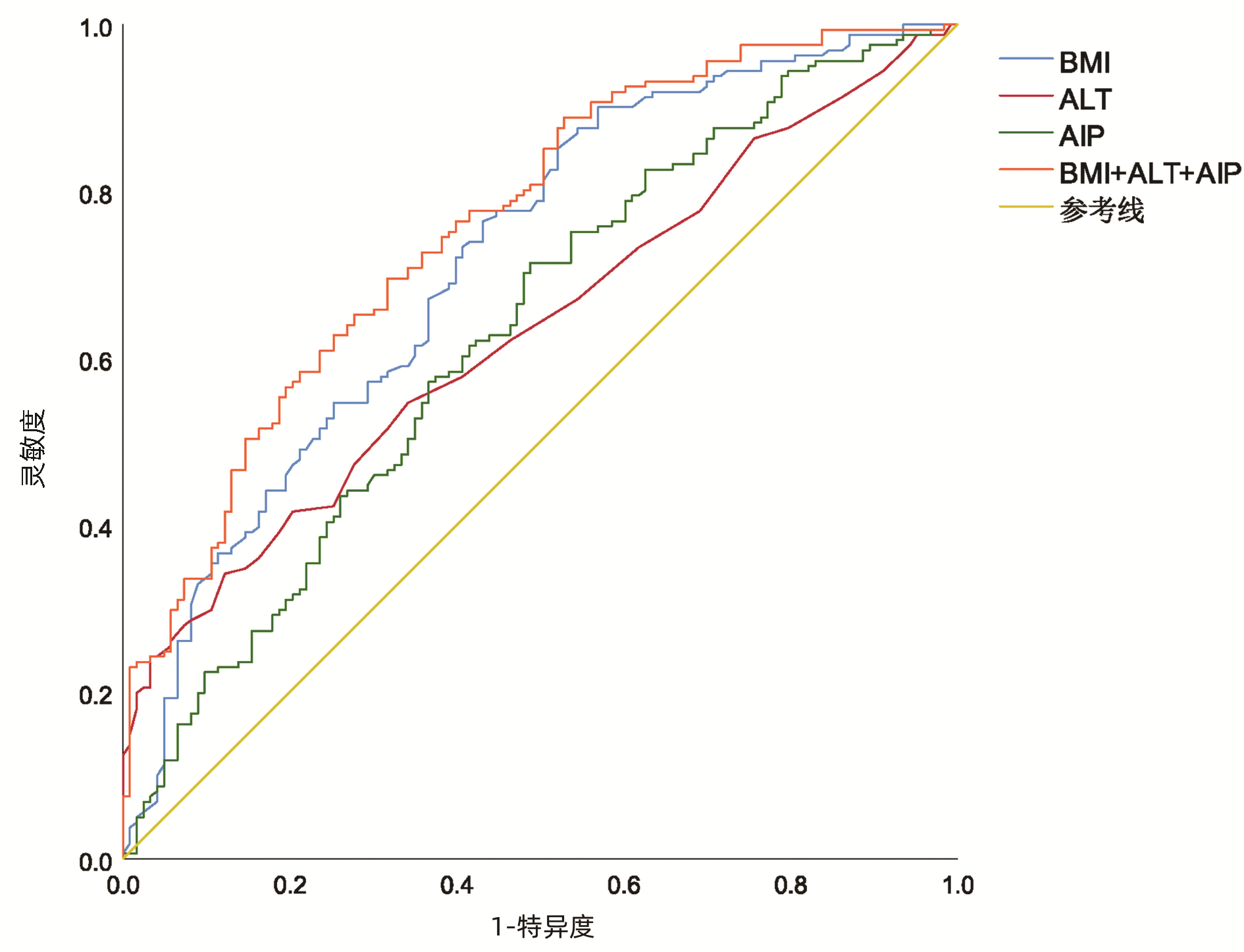
图 3 BMI<28 kg/m2组AIP、BMI、ALT及三者联合预测T2DM合并MAFLD的ROC曲线
Figure 3. ROC curves of AIP, BMI, ALT and their combination for predicting T2DM with MAFLD in BMI < 28 kg/m2 group
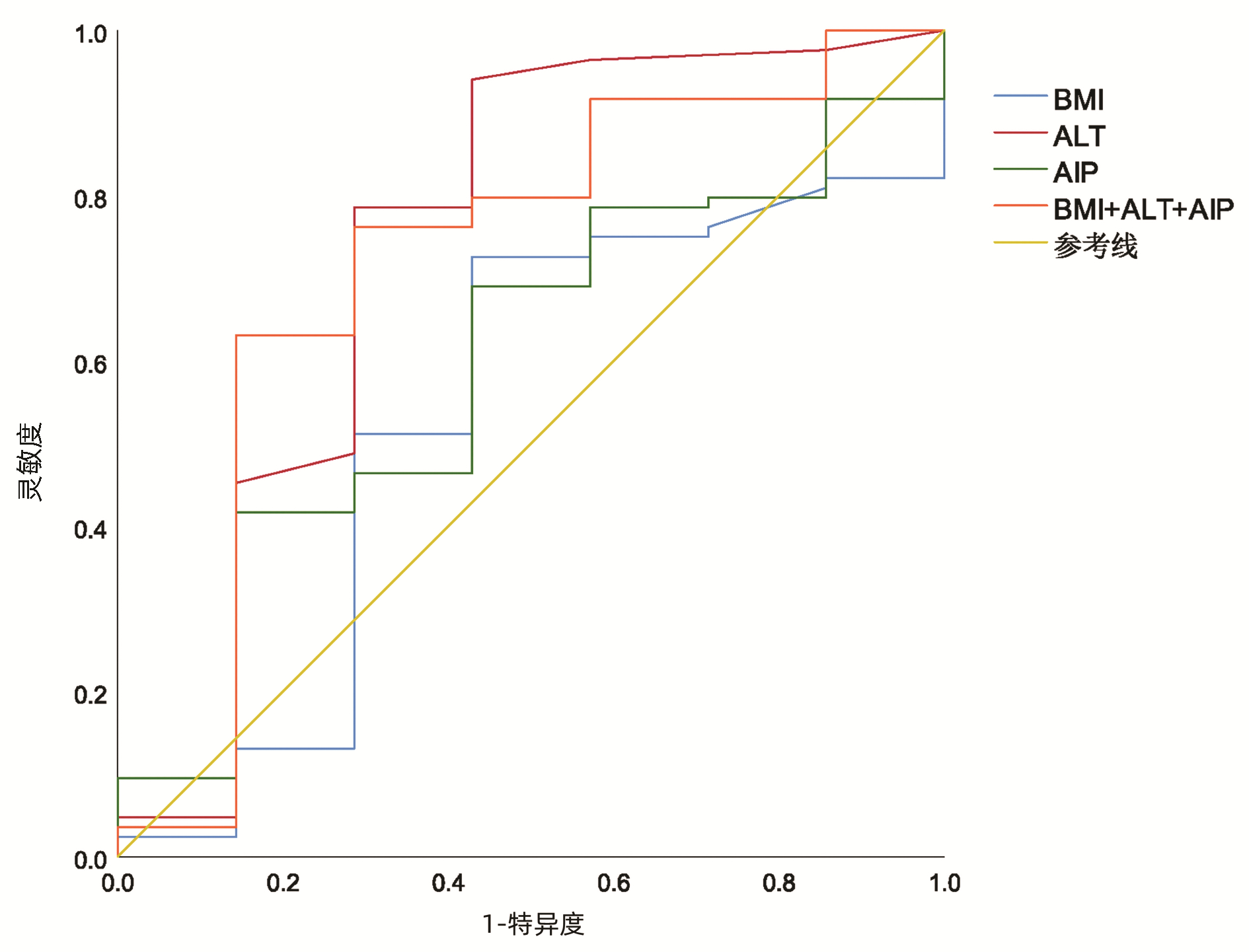
图 4 28 kg/m2≤BMI<40 kg/m2组AIP、BMI、ALT及三者联合预测T2DM合并MAFLD的ROC曲线
Figure 4. ROC curves of AIP, BMI, ALT and their combination for predicting T2DM with MAFLD in 28 kg/m2≤ BMI < 40 kg/m2
表 1 MAFLD与非MAFLD组的临床资料比较
Table 1. Comparison of clinical data between MAFLD and non-MAFLD groups
指标 T2DM组(n=130) T2DM+MAFLD组(n=245) 统计值 P值 T2DM病程(年) 1(0~3) 1(0~4) Z=-1.415 0.157 年龄(岁) 49(41~55) 47(38~55) Z=-0.837 0.403 性别(男/女,例) 74/56 150/95 χ2=0.653 0.419 BMI(kg/m2) 23.03(21.38~24.97) 26.57(24.07~28.99) Z=-8.966 <0.001 SBP(mmHg) 125(117~131) 126(122~134) Z=-3.272 0.001 DBP(mmHg) 78(75~80) 79(75~86) Z=-2.034 0.042 FBG(mmol/L) 6.6(5.7~7.5) 7.0(6.2~8.1) Z=-3.799 <0.001 HbA1C(%) 8.0(6.8~10.3) 8.9(7.3~10.5) Z=-2.346 0.019 2hPG(mmol/L) 14.44±4.25 14.79±3.70 t=0.837 0.403 UA(μmol/L) 264.97±76.69 305.60±84.56 t=4.490 <0.001 ALT(U/L) 15(11~21) 22(14~36) Z=-6.089 <0.001 AST(U/L) 15(12~18) 18(14~25) Z=-5.302 <0.001 GGT(U/L) 16(12~15) 27(18~41) Z=-7.203 <0.001 ALP(U/L) 71(59~85) 77(66~92) Z=-2.766 0.006 TC(mmol/L) 4.53±1.11 4.64±1.06 t=0.897 0.370 TG(mmol/L) 1.34(0.92~2.18) 1.85(1.28~3.06) Z=-4.674 <0.001 HDL-C(mmol/L) 1.01(0.88~1.24) 0.95(0.81~1.08) Z=1.422 0.035 LDL-C(mmol/L) 2.66±0.80 2.93±0.77 t=3.148 0.002 AIP 0.12(-0.09~0.36) 0.28(0.10~0.53) Z=4.742 <0.001 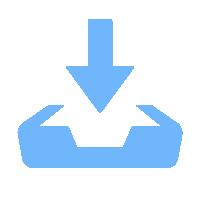 下载: 导出CSV
下载: 导出CSV
表 2 AIP与T2DM合并MAFLD发生关系的多因素Logistic回归分析
Table 2. Multivariate Logistic regression analysis of the relationship between AIP and MAFLD
组别 模型1 模型2 模型3 OR (95%CI) P值 OR (95%CI) P值 OR (95%CI) P值 Q1组 1.000 1.000 1.000 Q2组 1.974(1.094~3.562) 0.024 1.658(0.845~3.252) 0.142 1.295(0.630~2.662) 0.481 Q3组 2.543(1.388~4.662) 0.003 1.566(0.776~3.162) 0.211 1.213(0.574~2.566) 0.613 Q4组 5.634(2.852~11.132) <0.001 3.954(1.774~8.815) 0.001 2.396(1.018~5.640) 0.045 注:模型1,未校正任何危险因素;模型2,校正T2DM病程、SBP、DBP、BMI; 模型3, 在模型2的基础上进一步调整FBG、HbA1C、LDL-C、ALT。
下载: 导出CSV
表 3 AIP、BMI、ALT预测T2DM合并MAFLD发生的ROC曲线分析
Table 3. ROC curve analysis of AIP, BMI and ALT predictingT2DM and MAFLD occurrence
变量 AUC 95%CI 最佳临界值 灵敏度(%) 特异度(%) P值 总人群 联合诊断模型 0.816 0.773~0.860 0.670 70.2 78.5 0.023 AIP 0.661 0.604~0.718 0.103 75.1 49.2 0.030 ALT 0.691 0.638~0.744 25.500 43.7 86.9 0.027 BMI 0.781 0.733~0.809 25.635 58.8 83.8 0.025 BMI<28 kg/m2 联合诊断模型 0.760 0.704~0.815 0.550 69.4 68.3 0.028 AIP 0.630 0.564~0.695 0.104 71.3 51.2 0.033 ALT 0.632 0.569~0.696 25.500 33.8 87.8 0.033 BMI 0.717 0.656~0.777 23.205 76.3 56.9 0.031 28 kg/m2≤BMI<40 kg/m2 联合诊断模型 0.741 0.507~0.976 0.885 82.4 71.4 0.035 AIP 0.597 0.388~0.805 0.469 41.2 85.7 0.397 ALT 0.742 0.494~0.990 11.500 94.1 57.1 0.034 BMI 0.541 0.308~0.775 28.930 72.9 57.1 0.119
下载: 导出CSV
-
[1] de ALWIS NM, DAY CP. Non-alcoholic fatty liver disease: the mist gradually clears[J]. J Hepatol, 2008, 48(Suppl 1): S104-S112. DOI: 10.1016/j.jhep.2008.01.009. [2] CHALASANI N, YOUNOSSI Z, LAVINE JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association[J]. Hepatology, 2012, 55(6): 2005-2023. DOI: 10.1002/hep.25762. [3] DOU KF, YANG XS. Surgeons should attach importance to the understanding of metabolic associated fatty liver disease[J]. Chin J Dig Surg, 2021, 20(1): 40-45. DOI: 10.3760/cma.j.cn115610-20201214-00780.窦科峰, 杨西胜. 外科医师应重视对代谢相关脂肪性肝病的认识[J]. 中华消化外科杂志, 2021, 20(1): 40-45. DOI: 10.3760/cma.j.cn115610-20201214-00780. [4] XUE R, FAN JG. Brief introduction of an international expert consensus statement: A new definition of metabolic associated fatty liver disease[J]. J Clin Hepatol, 2020, 36(6): 1224-1227. DOI: 10.3969/j.issn.1001-5256.2020.06.007.薛芮, 范建高. 代谢相关脂肪性肝病新定义的国际专家共识简介[J]. 临床肝胆病杂志, 2020, 36(6): 1224-1227. DOI: 10.3969/j.issn.1001-5256.2020.06.007. [5] YOUNOSSI ZM, GOLABI P, de AVILA L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis[J]. J Hepatol, 2019, 71(4): 793-801. DOI: 10.1016/j.jhep.2019.06.021. [6] FERNÁNDEZ-MACÍAS JC, OCHOA-MARTÍNEZ AC, VARELA-SILVA JA, et al. Atherogenic index of plasma: Novel predictive biomarker for cardiovascular illnesses[J]. Arch Med Res, 2019, 50(5): 285-294. DOI: 10.1016/j.arcmed.2019.08.009. [7] CHANG Y, LI Y, GUO X, et al. The association of ideal cardiovascular health and atherogenic index of plasma in rural population: A cross-sectional study from Northeast China[J]. Int J Environ Res Public Health, 2016, 13(10): 1027. DOI: 10.3390/ijerph13101027. [8] LIU H, LIU K, PEI L, et al. Atherogenic index of plasma predicts outcomes in acute ischemic stroke[J]. Front Neurol, 2021, 12: 741754. DOI: 10.3389/fneur.2021.741754. [9] World Health Organization. Definition, diagnosis and classification of diabetes mellitus and its complications: report of a WHO consultation. Part 1, Diagnosis and classification of diabetes mellitus[R]. World health organization, 1999. [10] XIE J, YANG M, XING Y. Effects of liraglutide on glucose and lipid metabolism and insulin resistance in type 2 diabetes mellitus patients with non-alcoholic fatty liver disease[J/CD]. Chin J Liver Dis (Electronic Version), 2021, 13(4): 46-53. DOI: 10.3969/j.issn.1674-7380.2021.04.008 .谢晶, 杨淼, 邢英. 利拉鲁肽对2型糖尿病合并非酒精性脂肪性肝病患者糖脂代谢及胰岛素抵抗的影响[J/CD]. 中国肝脏病杂志(电子版), 2021, 13(4): 46-53. DOI:10.3969/j.issn.1674-7380.2021.04.008 .[11] ZHOU F, ZHOU J, WANG W, et al. Unexpected rapid increase in the burden of NAFLD in China From 2008 to 2018: A systematic review and meta-analysis[J]. Hepatology, 2019, 70(4): 1119-1133. DOI: 10.1002/hep.30702. [12] DEWIDAR B, KAHL S, PAFILI K, et al. Metabolic liver disease in diabetes - From mechanisms to clinical trials[J]. Metabolism, 2020, 111S: 154299. DOI: 10.1016/j.metabol.2020.154299. [13] XIE F, ZHOU H, WANG Y. Atherogenic index of plasma is a novel and strong predictor associated with fatty liver: a cross-sectional study in the Chinese Han population[J]. Lipids Health Dis, 2019, 18(1): 170. DOI: 10.1186/s12944-019-1112-6. [14] SAMIMI S, RAJABZADEH S, RABIZADEH S, et al. Atherogenic index of plasma is an independent predictor of metabolic-associated fatty liver disease in patients with type 2 diabetes[J]. Eur J Med Res, 2022, 27(1): 112. DOI: 10.1186/s40001-022-00731-x. [15] SCHREUDER TC, VERWER BJ, van NIEUWKERK CM, et al. Nonalcoholic fatty liver disease: an overview of current insights in pathogenesis, diagnosis and treatment[J]. World J Gastroenterol, 2008, 14(16): 2474-2486. DOI: 10.3748/wjg.14.2474. [16] STEFAN N, KANTARTZIS K, HÄRING HU. Causes and metabolic consequences of fatty liver[J]. Endocr Rev, 2008, 29(7): 939-960. DOI: 10.1210/er.2008-0009. [17] POSTIC C, GIRARD J. Contribution of de novo fatty acid synthesis to hepatic steatosis and insulin resistance: lessons from genetically engineered mice[J]. J Clin Invest, 2008, 118(3): 829-838. DOI: 10.1172/JCI34275. [18] ABBASI F, REAVEN GM. Comparison of two methods using plasma triglyceride concentration as a surrogate estimate of insulin action in nondiabetic subjects: triglycerides×glucose versus triglyceride/high-density lipoprotein cholesterol[J]. Metabolism, 2011, 60(12): 1673-1676. DOI: 10.1016/j.metabol.2011.04.006. [19] DONG BY, MAO YQ, LI ZY, et al. The value of the atherogenic index of plasma in non-obese people with non-alcoholic fatty liver disease: a secondary analysis based on a cross-sectional study[J]. Lipids Health Dis, 2020, 19(1): 148. DOI: 10.1186/s12944-020-01319-2. [20] FRACANZANI AL, PETTA S, LOMBARDI R, et al. Liver and cardiovascular damage in patients with lean nonalcoholic fatty liver disease, and association with visceral obesity[J]. Clin Gastroenterol Hepatol, 2017, 15(10): 1604-1611. e1. DOI: 10.1016/j.cgh.2017.04.045. [21] GAWRIEH S, WILSON LA, CUMMINGS OW, et al. Histologic findings of advanced fibrosis and cirrhosis in patients with nonalcoholic fatty liver disease who have normal aminotransferase levels[J]. Am J Gastroenterol, 2019, 114(10): 1626-1635. DOI: 10.14309/ajg.0000000000000388. [22] CHEN JF, QIN Q, WU ZQ, et al. A cohort study on the correlation between alanine aminotransferase trajectories and new-onset metabolic fatty liver disease[J]. Chin J Epidemiol, 2022, 43(2): 234-240. DOI: 10.3760/cma.j.cn112338-20210809-00621.陈静锋, 秦迁, 吴卓青, 等. 谷丙转氨酶轨迹与新发代谢相关脂肪性肝病相关性的队列研究[J]. 中华流行病学杂志, 2022, 43(2): 234-240. DOI: 10.3760/cma.j.cn112338-20210809-00621. -

 本文二维码
本文二维码
计量
- 文章访问数: 219
- HTML全文浏览量: 129
- PDF下载量: 38
- 被引次数: 0

