
 PDF下载 ( 2228 KB)
PDF下载 ( 2228 KB)

五种评分系统预测高甘油三酯血症性急性胰腺炎严重程度的比较
DOI: 10.3969/j.issn.1001-5256.2023.06.020
Value of five scoring systems in predicting the severity of hyperlipidemic acute pancreatitis: A comparative analysis
-
摘要:
目的 探讨PASS评分、BISAP评分、APACHE-Ⅱ评分、HAPS评分和Ranson评分五种评分系统对高甘油三酯血症性急性胰腺炎(HTGAP)病情和预后评估的价值。 方法 回顾性分析宁夏医科大学总医院2016年1月—2022年1月收治的300例HTGAP患者的临床资料,根据患者病情程度分为轻症急性胰腺炎、中度重症急性胰腺炎、重症急性胰腺炎三个组别,比较三组患者的临床资料和评分系统差异,计数资料组间比较采用χ2检验,正态方差齐的计量资料采用方差分析,非正态分布的计量资料三组间比较采用Kruskal-Wallis H检验。根据病情程度是否重症,绘制受试者工作特征曲线(ROC曲线),比较指标的ROC曲线下面积(AUC)。 结果 三组间PASS评分(χ2=219.351)、Ranson评分(χ2=83.084)、APACHE-Ⅱ评分(χ2=43.388)和BISAP评分(χ2=50.785)差异均有统计学意义(P值均<0.01)。在病情严重程度的评估和预测方面, PASS评分的敏感度(0.945)和AUC(0.963)高于其他四种评分系统,Ranson评分的敏感度(0.655)和AUC(0.819)次之。 结论 对于HTGAP患者,PASS评分可以更准确地评估HTGAP患者的病情严重程度及预后,有望在临床中更好的推广应用。 -
关键词:
- 胰腺炎, 急性坏死性 /
- 高甘油三酯血症 /
- 疾病严重程度指数
Abstract:Objective To investigate the value of pancreatitis activity scoring system (PASS) score, Bedside Index for Severity in Acute Pancreatitis (BISAP) score, Acute Physiology and Chronic Health Evaluation Ⅱ (APACHE-Ⅱ) score, harmless acute pancreatitis score (HAPS), and Ranson score in evaluating the severity and prognosis of hypertriglyceridemia acute pancreatitis (HTGAP). Methods A retrospective analysis was performed for the clinical data of 300 patients with HTGAP who were admitted to General Hospital of Ningxia Medical University from January 2016 to January 2022, and according to the disease severity, these patients were divided into mild acute pancreatitis (MAP) group, moderate-severe acute pancreatitis (MSAP) group, and severe acute pancreatitis (SAP) group. Clinical data and the above scores were compared between the three groups. The chi-square test was used for comparison of categorical data between groups; an analysis of variance was used for continuous data with homogeneity of variance, and the Kruskal-Wallis H test was used for comparison of non-normally distributed continuous data between groups. The receiver operating characteristic (ROC) curve was plotted according to disease severity, and related indicators were compared in terms of the area under the ROC curve (AUC). Results There were significant differences between the three groups in PASS score (F=219.351, P < 0.01), Ranson score (χ2=83.084, P < 0.01), APACHE-Ⅱ score (χ2=43.388, P < 0.01), and BISAP score (χ2= 50.785, P < 0.01). Compared with the other four scoring systems in evaluating and predicting disease severity, PASS score had the highest sensitivity of 0.945 and the largest AUC of 0.963, followed by Ranson score with a sensitivity of 0.655 and an AUC of 0.819. Conclusion For patients with HTGAP, PASS score can more accurately assess the severity and prognosis of HTGAP patients and thus holds promise for clinical application. -
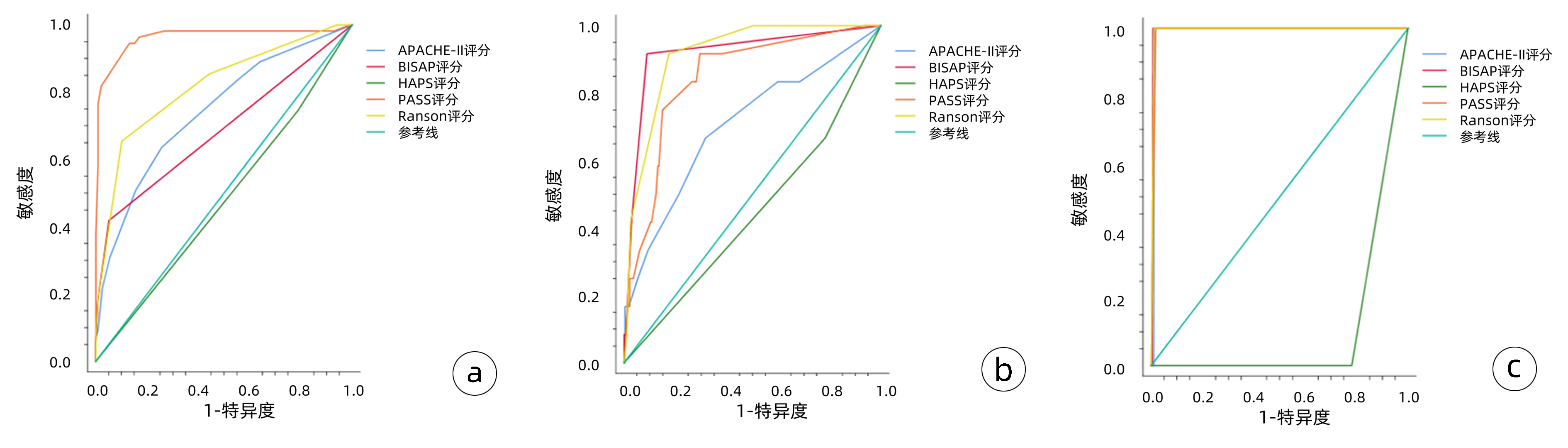
图 1 五种评分系统的ROC曲线
注:a,预测患者病情严重程度;b,预测患者并发症(胸腔积液);c,预测患者死亡。
Figure 1. ROC curves of the five scoring systems
表 1 3组患者一般情况比较
Table 1. Comparison of the general information among the three groups
指标 MAP(n=199) MSAP(n=48) SAP(n=53) 统计值 P值 年龄(岁) 35.0(30.0~40.0) 37.0(29.5~45.0) 36.0(31.3~42.8) χ2=2.518 0.284 BMI(kg/m2) 26.29(23.86~29.27) 27.34(25.47~28.52) 26.74(24.13~29.42) χ2=2.180 0.336 呼吸(次/min) 20(20~21) 21(20~21) 21(20~21) χ2=15.989 <0.001 心率(次/min) 26.74±4.48 26.50±4.46 36.21±8.61 F=0.608 0.545 性别[例(%)] χ2=1.263 0.540 男 167(83.9) 36(75.0) 44(83.0) 女 32(16.1) 12(25.0) 9(17.0) 吸烟[例(%)] 93(46.7) 23(47.9) 20(37.7) χ2=2.906 0.241 饮酒[例(%)] 80(40.2) 23(47.9) 21(39.6) χ2=2.180 0.349 药物服用史[例(%)] 39(19.6) 5(10.4) 13(24.5) χ2=2.531 0.286 合并脂肪肝[例(%)] 145(72.9) 38(79.2) 38(71.7) χ2=3.701 0.160 合并糖尿病[例(%)] 57(28.6) 16(33.3) 27(50.9) χ2=7.507 0.024 合并呼吸衰竭[例(%)] 0(0.0) 1(2.1) 4(7.5) χ2=11.241 0.002 合并高血压病[例(%)] 19(9.5) 5(10.4) 6(11.3) χ2=0.300 0.880 合并代谢性酸中毒[例(%)] 0(0.0) 1(2.1) 4(7.5) χ2=11.241 0.002 合并SIRS[例(%)] 0(0.0) 0(0.0) 4(7.5) χ2=11.139 0.002 合并脓毒症[例(%)] 0(0.0) 0(0.0) 4(7.5) χ2=11.139 0.002 合并MODS[例(%)] 0(0.0) 0(0.0) 4(7.5) χ2=11.139 0.002 合并胸腔积液[例(%)] 1(0.5) 3(6.3) 8(15.1) χ2=19.961 <0.001 合并腹腔积液[例(%)] 2(1.0) 0(0.0) 2(3.8) χ2=2.331 0.265 代谢综合征[例(%)] 5(2.5) 2(4.2) 1(1.9) χ2=0.958 0.749 注:SIRS,全身炎症反应综合征;MODS,多器官功能障碍综合征。  下载: 导出CSV
下载: 导出CSV
表 2 三组患者实验室检验结果比较
Table 2. Comparison of laboratory results among the three groups
指标 MAP(n=199) MSAP(n=48) SAP(n=53) 统计值 P值 WBC(×109/L) 110.41±18.41 20.78±1.09 22.05±3.69 F=9.424 <0.001 NEUT#(%) 100.44±74.12 20.90±2.36 20.61±1.97 F=10.758 <0.001 LYM(×109/L) 1.520(1.180~2.210) 1.410(1.115~1.920) 1.250(0.800~1.620) χ2=11.328 0.003 MXD(×109/L) 0.705(0.520~0.900) 0.700(0.570~1.000) 0.690(0.553~0.983) χ2=1.486 0.476 PTL(×109/L) 7.35±0.09 105.09±15.74 110.41±18.42 F=1.544 0.215 HCT(%) 45.70(42.80~48.40) 46.70(43.30~49.20) 46.95(41.55~50.60) χ2=1.959 0.376 D-dimer(μg/mL) 0.30(0.20~0.64) 0.32(0.20~0.76) 0.82(0.34~1.96) χ2=25.235 <0.001 PT(s) 11.00(10.00~11.00) 11.20(10.15~11.75) 11.80(10.80~13.00) χ2=19.045 <0.001 INR 0.95(0.89~1.00) 0.960(0.865~1.025) 1.02(0.94~1.12) χ2=25.617 <0.001 GLU(mmol/L) 8.235(6.190~12.163) 9.440(6.895~14.325) 12.770(9.325~17.588) χ2=27.509 <0.001 Ca(mmol/L) 2.310(2.210~2.390) 2.250(2.090~2.360) 2.060(1.785~2.218) χ2=45.766 <0.001 K(mmol/L) 4.165(3.948~4.445) 4.210(3.910~4.350) 4.150(3.905~4.810) χ2=0.613 0.736 BUN(mmol/L) 4.275(3.450~5.393) 4.320(3.645~5.285) 5.390(3.915~6.635) χ2=11.603 0.003 CREA(μmol/L) 61.900(54.100~71.300) 58.600(51.350~68.950) 62.000(50.025~83.750) χ2=2.224 0.329 UA(μmol/L) 405.50(346.75~484.25) 375.00(329.50~480.50) 414.00(307.00~493.00) χ2=0.516 0.773 Alb(g/L) 43.850(40.780~46.930) 42.800(39.500~46.900) 38.700(34.350~43.025) χ2=24.657 <0.001 LDH(U/L) 531.00(432.25~633.25) 659.00(513.50~819.00) 780.00(480.75~1 268.75) χ2=39.743 <0.001 TC(mmol/L) 6.880(5.770~8.520) 7.460(6.200~10.425) 7.000(6.268~9.540) χ2=2.885 0.236 TG(mmol/L) 12.635(10.770~21.683) 11.860(11.850~24.975) 13.910(8.503~27.740) χ2=0.669 0.716 AMY(U/L) 196.00(90.75~358.00) 292.00(140.50~440.00) 411.00(190.00~607.50) χ2=17.024 <0.001 LIP(U/L) 1 161.5(434.0~3 641.0) 922.0(554.0~3 109.5) 2 283.0(1 016.0~5 589.0) χ2=9.880 0.007 CRP(mg/L) 89.00(45.00~136.00) 136.00(79.75~273.75) 154.50(90.00~255.50) χ2=28.317 <0.001
下载: 导出CSV
表 3 三组患者评分系统和疾病转归及预后比较
Table 3. Comparison of scoring systems, disease outcome, and prognosis among the three groups of patients
指标 MAP(n=199) MSAP(n=48) SAP(n=53) χ2值 P值 PASS评分 90.0(90.0~90.0) 140.0(115.0~140.0) 200.0(152.5~220.0) 219.351 <0.001 Ranson评分 1(1~2) 2(2~2) 2(2~2) 83.084 <0.001 HAPS评分 1(1~1) 1(1~1) 1(0~1) 0.480 0.799 APACHE-Ⅱ评分 1(1~1) 1(1~2) 2(1~2) 43.388 <0.001 BISAP评分 0(0~0) 0(0~0) 0(0~1) 50.785 <0.001 住院天数(d) 7.00(4.00~9.00) 11.00(8.00~14.50) 10.00(6.25~15.75) 48.281 <0.001 住院费用(元) 10 713(7 200~17 224) 17 027(11 800~24 020) 31 189(21 395~47 700) 93.894 <0.001 ICU[例(%)] 0(0.0) 0(0.0) 6(11.3) 17.317 <0.001 死亡[例(%)] 0(0.0) 0(0.0) 1(1.9) 3.662 0.338 复发[例(%)] 91(45.7) 14(29.2) 36(67.9) 11.357 0.003
下载: 导出CSV
表 4 五种评分系统对HTGAP患者病情严重程度、并发症和死亡的评估准确性比较
Table 4. Comparison of the accuracy of the five scoring systems in evaluating patients' severity of disease, complications, and mortality
评分系统及预后指标 AUC P值 敏感度 特异度 阳性预测值 阳性似然比 约登指数 APACHE-Ⅱ MSAP、SAP 0.744 <0.001 0.636 0.743 0.712 2.472 0.379 胸腔积液 0.704 0.016 0.683 0.350 0.678 2.105 0.350 死亡 0.990 <0.001 1.000 0.990 0.990 97.333 0.990 BISAP MSAP、SAP 0.687 <0.001 0.418 0.949 0.892 8.259 0.368 胸腔积液 0.919 <0.001 0.917 0.911 0.912 10.303 0.828 死亡 0.995 <0.001 1.000 0.993 0.993 146.000 0.993 PASS MSAP、SAP 0.963 <0.001 0.945 0.869 0.878 7.288 0.815 胸腔积液 0.846 <0.001 0.917 0.705 0.756 3.103 0.621 死亡 0.991 <0.001 1.000 0.983 0.983 58.400 0.983 Ranson MSAP、SAP 0.819 <0.001 0.655 0.899 0.866 6.464 0.553 胸腔积液 0.916 <0.001 0.917 0.826 0.840 5.257 0.742 死亡 0.995 <0.001 1.000 0.990 0.990 97.333 0.990 HAPS MSAP、SAP 0.418 0.619 0.745 0.211 0.486 0.945 -0.044 胸腔积液 0.442 0.512 0.512 0.217 0.460 0.852 -0.016 死亡 0.110 <0.001 0.000 0.219 0.000 0.000 -0.781
下载: 导出CSV
-
[1] HE WH, ZHU Y. Diagnosis and lipid-lowering treatment strategy for hypertriglyceridemic pancreatitis[J]. Chin J Pancreatol, 2022, 22(4): 241-246. DOI: 10.3760/cma.j.cn115667-20220711-00098.何文华, 祝荫. 高三酰甘油血症性胰腺炎的诊断和降脂治疗策略[J]. 中华胰腺病杂志, 2022, 22(4): 241-246. DOI: 10.3760/cma.j.cn115667-20220711-00098. [2] SU W, GUO F. Triglyceride-controlling during acute phase of hypertriglyceridemia induced pancreatitis[J]. Chin J Dig Surg, 2023, 22(1): 89-93. DOI: 10.3760/cma.j.cn115610-20221220-00755.苏伟, 郭丰. 高甘油三酯血症性胰腺炎急性期的血脂控制[J]. 中华消化外科杂志, 2023, 22(1): 89-93. DOI: 10.3760/cma.j.cn115610-20221220-00755. [3] DU YQ, SONG YX. Characteristics and treatment of hypertriglyceridemia acute pancreatitis[J]. Chin J Pract Int Med, 2021, 41(1): 10-13. DOI: 10.19538/j.nk2021010103.杜奕奇, 宋英晓. 高三酰甘油血症急性胰腺炎的特点与处理[J]. 中国实用内科杂志, 2021, 41(1): 10-13. DOI: 10.19538/j.nk2021010103. [4] Pancreas Study Group, Chinese Society of Gastroenterology, Chinese Medical Association, Editorial Board of Chinese Journal of Pancreatology, Editorial Board of Chinese Journal of Digestion. Chinese guidelines for the management of acute pancreatitis (Shenyang, 2019)[J]. J Clin Hepatol, 2019, 35(12): 2706-2711. DOI: 10.3969/j.issn.1001-5256.2019.12.013.中华医学会消化病学分会胰腺疾病学组, 《中华胰腺病杂志》编委会, 《中华消化杂志》编委会. 中国急性胰腺炎诊治指南(2019年, 沈阳)[J]. 临床肝胆病杂志, 2019, 35(12): 2706-2711. DOI: 10.3969/j.issn.1001-5256.2019.12.013. [5] WU BU, JOHANNES RS, SUN X, et al. The early prediction of mortality in acute pancreatitis: a large population-based study[J]. Gut, 2008, 57(12): 1698-1703. DOI: 10.1136/gut.2008.152702. [6] TANG YF, TANG GD, LIANG ZH, et al. Clinical features of severe acute hypertriglyceridemic pancreatitis[J]. J Clin Hepatol, 2019, 35(4): 830-834. DOI: 10.3969/j.issn.1001-5256.2019.04.024.唐永凤, 唐国都, 梁志海, 等. 重症高甘油三酯性急性胰腺炎的临床特征分析[J]. 临床肝胆病杂志, 2019, 35(4): 830-834. DOI: 10.3969/j.issn.1001-5256.2019.04.024. [7] ZHAO HJ, WU D, WU WM, et al. Research advances of hyperlipidemic pancreatitis[J]. Med J Pumch, 2022, 13(4): 637-643. DOI: 10.12290/xhyxzz.2021-0760.赵慧佳, 吴东, 吴文铭, 等. 高脂血症性胰腺炎研究进展[J]. 协和医学杂志, 2022, 13(4): 637-643. DOI: 10.12290/xhyxzz.2021-0760. [8] CHEN HZ, JI L, LI L, et al. Early prediction of infected pancreatic necrosis secondary to necrotizing pancreatitis[J]. Medicine (Baltimore), 2017, 96(30): e7487. DOI: 10.1097/MD.0000000000007487. [9] WU BU, BATECH M, QUEZADA M, et al. Dynamic measurement of disease activity in acute pancreatitis: the pancreatitis activity scoringsystem[J]. Am J Gastroenterol, 2017, 112(7): 1144-1152. DOI: 10.1038/ajg.2017.114. [10] BUXBAUM J, QUEZADA M, CHONG B, et al. The Pancreatitis Activity Scoring System predicts clinical outcomes in acute pancreatitis: findings from a prospective cohort study[J]. Am J Gastroenterol, 2018, 113(5): 755-764. DOI: 10.1038/s41395-018-0048-1. [11] YU Z, NI Q, ZHANG P, et al. Clinical utility of the pancreatitis activity scoring system in severe acute pancreatitis[J]. Front Physiol, 2022, 13: 935329. DOI: 10.3389/fphys.2022.935329. [12] ONG Y, SHELAT VG. Ranson score to stratify severity in acute pancreatitis remains valid-old is gold[J]. Expert Rev Gastroenterol Hepatol, 2021, 15(8): 865-877. DOI: 10.1080/17474124.2021.1924058. [13] MIKÓ A, VIGH É, MÁTRAI P, et al. Computed tomography severity index vs. other indices in the prediction of severity and mortality in acute pancreatitis: A predictive accuracy meta-analysis[J]. Front Physiol, 2019, 10: 1002. DOI: 10.3389/fphys.2019.01002. [14] HE WH, ZHENG X, ZHU Y, et al. To study the early prediction method of acute pancreatitis severity and infectious pancreatic necrosis based on acute pancreatitis database[J]. Chin J Pancreatol, 2019, 19(3): 172- 176. DOI: 10.3760/cma.j.issn.1674-1935.2019.03.004.何文华, 郑西, 祝荫, 等. 基于大样本数据库比较APACHEⅡ、Ranson、BISAP和CTSI评分在早期预测急性胰腺炎病情严重程度的价值[J]. 中华胰腺病杂志, 2019, 19(3): 172-176. DOI: 10.3760/cma.j.issn.1674-1935.2019.03.004. [15] HAN T, CHENG T, LIAO Y, et al. Thrombo-inflammatory prognostic scores improve bisap-based risk stratification in acute pancreatitis patients: A retrospective cohort study[J]. J Inflamm Res, 2022, 15: 3323-3335. DOI: 10.2147/JIR.S366246. [16] VALVERDE-LÓPEZ F, MATAS-COBOS AM, ALEGRÍA-MOTTE C, et al. BISAP, RANSON, lactate and others biomarkers in prediction of severe acute pancreatitis in a European cohort[J]. J Gastroenterol Hepatol, 2017, 32(9): 1649-1656. DOI: 10.1111/jgh.13763. [17] GAO W, YANG HX, MA CE. The value of BISAP score for predicting mortality and severity in acute pancreatitis: A systematic review and meta-analysis[J]. PLoS One, 2015, 10(6): e0130412. DOI: 10.1371/journal.pone.0130412. [18] LUO XP, WANG J, WU Q, et al. Research advances in acute pancreatitis scoring system[J]. J Clin Hepatol, 2022, 38(9): 2188-2192. DOI: 10.3969/j.issn.1001-5256.2022.09.046.罗秀平, 王洁, 吴青, 等. 急性胰腺炎评分系统的研究进展[J]. 临床肝胆病杂志, 2022, 38(9): 2188-2192. DOI: 10.3969/j.issn.1001-5256.2022.09.046. [19] MA XH, LI L, JIN T, et al. Harmless acute pancreatitis score on admission can accurately predict mild acute pancreatitis[J]. J South Med Univ, 2020, 40(2): 190-195. DOI: 10.12122/j.issn.1673-4254.2020.02.09.马小华, 李兰, 金涛, 等. 入院时无害性急性胰腺炎评分可预测轻症急性胰腺炎[J]. 南方医科大学学报, 2020, 40(2): 190-195. DOI: 10.12122/j.issn.1673-4254.2020.02.09. -

 本文二维码
本文二维码
计量
- 文章访问数: 272
- HTML全文浏览量: 42
- PDF下载量: 34
- 被引次数: 0

