
 PDF下载 ( 2570 KB)
PDF下载 ( 2570 KB)

血清IL-6和TNF-α对重症急性胰腺炎的早期诊断价值分析
DOI: 10.3969/j.issn.1001-5256.2023.07.020
Value of serum interleukin-6 and tumor necrosis factor-α in early diagnosis of severe acute pancreatitis
-
摘要:
目的 评估血清细胞因子在重症急性胰腺炎(SAP)早期诊断中的价值, 并利用LASSO算法构建复合指标的数理模型以提高对SAP诊断的准确性。 方法 纳入2019年1月-2022年6月在常熟市第一人民医院就诊的130例急性胰腺炎患者, 其中SAP患者73例, 非SAP患者57例。收集所有患者的外周血清样本并通过Luminex xMAP液相芯片技术完成13种血清细胞因子的精准检测。同时, 所有患者均进行APACHE Ⅱ、BISAP和CTSI评分。使用Kolmogorov-Smirnov法进行正态性检验, 对符合正态分布的计量资料两组间比较采用成组t检验; 对非正态分布的计量资料两组间比较采用Mann-Whitney U检验。计数资料两组间比较采用χ2检验。此外, 通过二元Logistic回归分析评估细胞因子对SAP的影响, 应用线性回归分析评估细胞因子与SAP疾病的严重程度之间的关联。偏相关分析在校正协变量(年龄、性别、BMI、高血压、糖尿病病史)后分析细胞因子与SAP疾病的严重程度评分的关联性。利用LASSO算法构建复合指标的数理模型, 并采用受试者工作特征曲线(ROC曲线)分析血清细胞因子对SAP临床诊断的效能, 计算曲线下面积(AUC)。 结果 非SAP组APACHE Ⅱ、BISAP和CTSI评分、改良Marshall评分均低于SAP组, 差异均有统计学意义(P值均 < 0.001)。SAP组患者IFN-γ、IL-1β、IL-6、IL-8、TNF-α水平均高于非SAP组, IL-12水平明显低于非SAP组, 差异均有统计学意义(P值均 < 0.05)。Logistic回归分析结果显示, IFN-γ(OR=1.190, 95%CI: 1.036~1.367, P=0.014)、IL-6(OR=1.148, 95%CI: 1.070~1.231, P < 0.001)和TNF-α(OR=1.100, 95%CI: 1.048~1.155, P < 0.001)为SAP的独立影响因素。偏相关分析提示, 在校正了性别、年龄、BMI、慢性疾病史(糖尿病、高血压)后, SAP患者IL-6和TNF-α的水平与APACHE Ⅱ评分均呈显著正相关(IL-6:r=0.503, P < 0.001;TNF-α: r=0.557, P < 0.001)。线性回归分析显示, SAP患者中IL-6和TNF-α水平均与APACHE Ⅱ评分有关(IL-6:β=0.049, P=0.044;TNF-α: β=0.054, P=0.046), 且IL-6和TNF-α存在交互作用, 影响APACHE Ⅱ评分。ROC曲线分析显示, LASSO算法联合IL-6和TNF-α构建的风险评分区分SAP和非SAP的AUC值最大(AUC=0.925), 而IL-6和TNF-α的AUC分别为0.885、0.878;偏相关分析发现, 在校正性别、年龄、BMI、慢性疾病史(糖尿病、高血压)后, SAP患者风险评分与APACHE Ⅱ评分呈显著正相关(r=0.565, P < 0.001)。 结论 血清IL-6和TNF-α水平可反映AP疾病严重程度。联合血清IL-6和TNF-α构建的风险评分可显著提高SAP早期诊断的准确性, 对SAP的临床诊疗具有重要的临床价值。 Abstract:Objective To investigate the value of serum cytokines in the early diagnosis of severe acute pancreatitis (SAP), and to improve the accuracy of the diagnosis of SAP by establishing a mathematical model with composite indices based on LASSO algorithm. Methods A total of 130 patients with acute pancreatitis (AP) who attended Changshu First People's Hospital from January 2019 to June 2022 were enrolled, among whom there were 73 SAP patients and 57 non-SAP patients.Peripheral serum samples were collected from all patients, and Luminex xMAP liquid chip technique was used to measure 13 serum cytokines.Meanwhile, Acute Physiology and Chronic Health Evaluation Ⅱ(APACHE Ⅱ), Bedside Index for Severity in Acute Pancreatitis (BISAP), and Computed Tomography Severity Index (CTSI) scores were determined for all patients.The Kolmogorov-Smirnov method was used for normality test; the independent-samples t test was used for comparison of normally distributed continuous data between two groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test was used for comparison of categorical data between two groups.Furthermore, the binary logistic regression analysis was used to evaluate the effect of cytokines on SAP, and the linear regression analysis was used to investigate the correlation between cytokines and SAP severity.The partial correlation analysis was used to evaluate the correlation between cytokines and SAP severity score after adjustment for covariates[age, sex, body mass index (BMI), and history of hypertension and diabetes].The LASSO algorithm was used to establish a mathematical model with composite indices; the receiver operating characteristic (ROC) curve was used to assess the performance of serum cytokines in the clinical diagnosis of SAP, and the area under the ROC curve (AUC) was calculated. Results Compared with the SAP group, the non-SAP group had significantly lower APACHE Ⅱ, BISAP, CTSI, and modified Marshall scores (all P < 0.001).Compared with the non-SAP group, the SAP group had significantly higher levels of interferon-γ(IFN-γ), interleukin-6(IL-6), interleukin-8, and tumor necrosis factor-α(TNF-α) and a significantly lower level of interleukin-12(all P < 0.05).The logistic regression analysis showed that IFN-γ(odds ratio[OR]=1.190, 95% confidence interval[CI]: 1.036-1.367, P=0.014), IL-6 (OR=1.148, 95%CI: 1.070-1.231, P < 0.001), and TNF-α (OR=1.100, 95%CI: 1.048-1.155, P < 0.001) were independent influencing factors for SAP.The partial correlation analysis showed that after adjustment for sex, age, BMI, and history of chronic diseases (diabetes and hypertension), the levels of IL-6 and TNF-α were positively correlated with APACHE Ⅱ score in SAP patients (IL-6:r=0.503, P < 0.001;TNF-α: r=0.557, P < 0.001).The linear regression analysis showed that the levels of IL-6 and TNF-α were associated with APACHE Ⅱ score in SAP patients (IL-6:β=0.049, P=0.044;TNF-α: β=0.054, P=0.046), and there was an interaction between IL-6 and TNF-α, which affected APACHE Ⅱ score.The ROC curve analysis showed that the risk score based on IL-6 and TNF-α using LASSO algorithm had the largest AUC of 0.925 in distinguishing SAP from non-SAP, while IL-6 or TNF-α alone had an AUC of 0.885 and 0.878, respectively.The partial correlation analysis showed that after adjustment for sex, age, BMI, and history of chronic diseases (diabetes and hypertension), the risk score was positively correlated with APACHE Ⅱ score in SAP patients (r=0.565, P < 0.001). Conclusion The serum levels of IL-6 and TNF-α can reflect the severity of AP.The risk score combining serum IL-6 and TNF-α can significantly improve the accuracy of the early diagnosis of SAP, which has an important clinical value in the clinical diagnosis and treatment of SAP. -
Key words:
- Pancreatitis /
- Interleukin-6 /
- Tumor Necrosis Factor-alpha /
- LASSO Algorithm
-
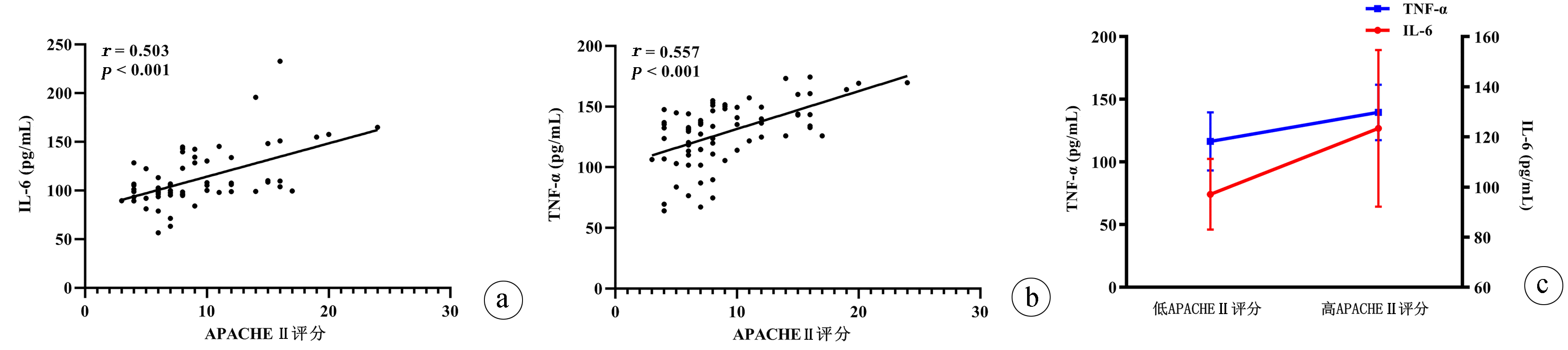
图 1 SAP组患者细胞因子水平与APACHE Ⅱ评分的关联分析
注:a,IL-6水平与APACHE Ⅱ评分的相关性;b,TNF-α水平与APACHE Ⅱ评分的相关性;c,IL-6和TNF-α水平交互作用对APACHE Ⅱ评分的影响(基于SAP患者APACHE Ⅱ评分的中位数分为低APACHE Ⅱ评分组和高APACHE Ⅱ评分组)。
Figure 1. Association of cytokine levels with APACHE Ⅱscore in SAP patients

图 2 IFN-γ、IL-6、TNF-α诊断SAP的ROC曲线分析
Figure 2. ROC curve analysis of IFN-γ、IL-6、TNF-α in diagnosis of severe acute pancreatitis
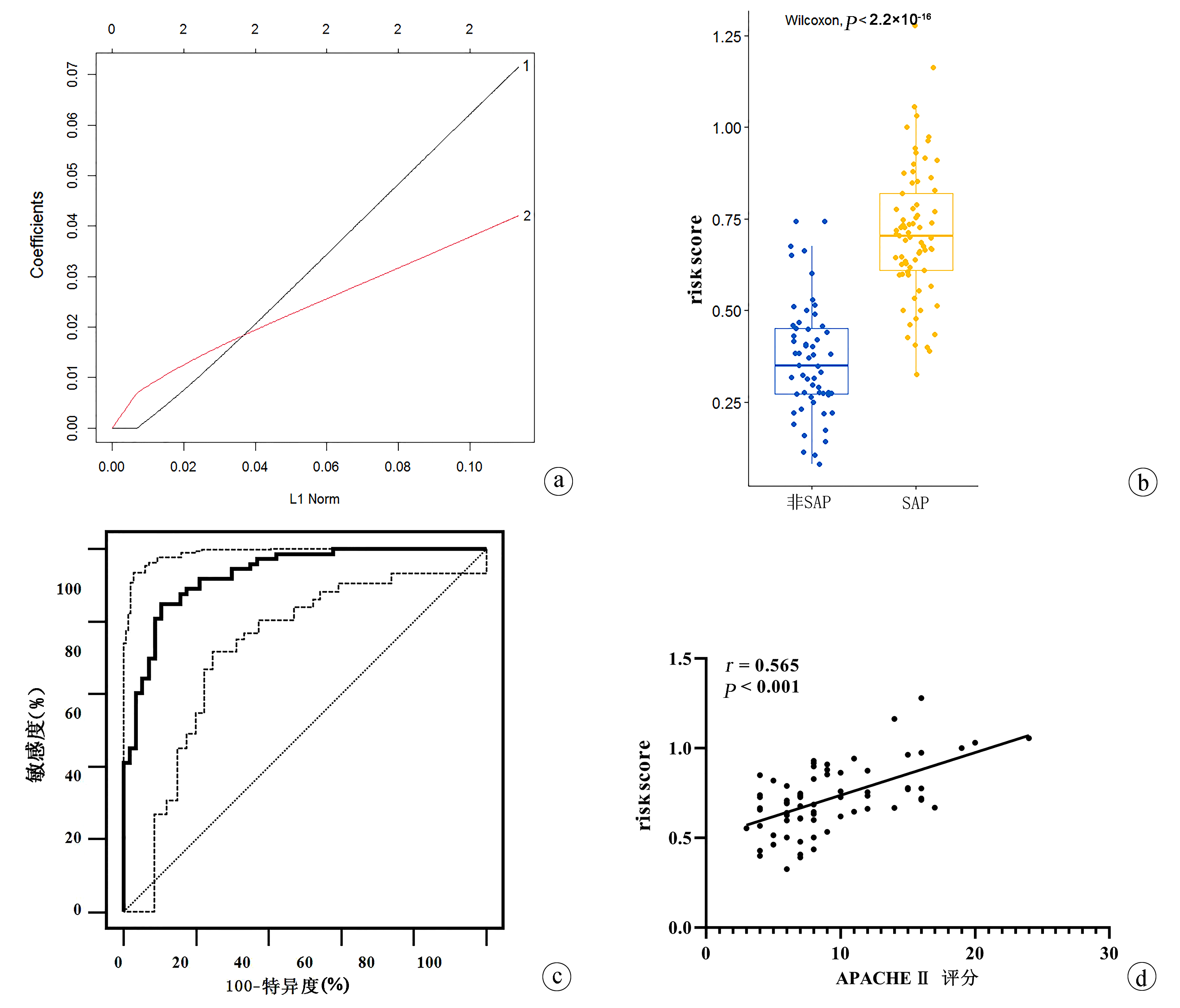
图 3 风险评分模型的构建及其对SAP的诊断价值
注:a,风险评分LASSO模型(黑线1:IL-6;红线2:TNF-α);b,风险评分的比较;c,诊断SAP的ROC曲线及95%CI;d,SAP组风险评分与APACHE Ⅱ评分的相关性。
Figure 3. Construction of risk scoring model and its diagnostic value for SAP
表 1 两组AP患者临床资料比较
Table 1. Comparison of clinical data between two groups of patients with AP
项目 非SAP组(n=57) SAP组(n=73) 统计值 P值 年龄(岁) 56.04±15.70 57.25±16.90 t=-0.418 0.676 男[例(%)] 28(49.12) 40(54.79) χ2=0.413 0.521 BMI(kg/m2) 22.44±3.56 23.31±3.14 t=-1.474 0.143 糖尿病[例(%)] 7(12.28) 15(20.55) χ2=1.556 0.212 高血压[例(%)] 16(28.07) 23(31.51) χ2=0.180 0.671 AP病因[例(%)] 胆源性 45(78.95) 51(69.86) χ2=1.368 0.242 高脂血症性 4(7.02) 11(15.07) χ2=2.033 0.154 酒精性 6(10.53) 7(9.59) χ2=0.031 0.860 病因不明 2(3.51) 4(5.48) χ2=0.282 0.595 APACHE Ⅱ评分 4(4~5) 8(6~12) Z=-7.503 <0.001 BISAP评分 2(1~2) 4(3~4) Z=-9.818 <0.001 CTSI评分 2(2~3) 6(5~7) Z=-9.797 <0.001 改良Marshall评分 1(0~2) 3(3~4) Z=-8.555 <0.001 循环衰竭[例(%)] 4(7.02) 25(34.25) 呼吸衰竭[例(%)] 10(17.54) 47(63.38) 肾衰竭[例(%)] 2(3.51) 8(10.96)  下载: 导出CSV
下载: 导出CSV
表 2 两组AP患者细胞因子水平的比较
Table 2. Comparison of cytokines levels in patients with SAP group and non-SAP group
细胞因子 非SAP(n=57) SAP(n=73) 统计值 P值 GM-CSF(pg/mL) 36.45±5.01 38.39±7.79 t=-1.638 0.104 IFN-γ(pg/mL) 38.69±7.11 42.26±11.96 t=-2.114 0.037 IL-1β(pg/mL) 12.93(10.09~16.60) 15.85(12.96~19.67) Z=-3.207 0.001 IL-2(pg/mL) 1.13(0.80~1.72) 1.20(0.98~1.79) Z=-1.185 0.236 IL-4(pg/mL) 38.76±7.22 40.12±5.65 t=-1.174 0.243 IL-5(pg/mL) 0.56(0.43~0.72) 0.59(0.47~0.76) Z=-1.159 0.246 IL-6(pg/mL) 69.12±24.01 110.81±27.78 t=-9.004 <0.001 IL-7(pg/mL) 5.16±2.55 5.33±2.39 t=-0.383 0.702 IL-8(pg/mL) 62.48±15.04 74.90±11.78 t=-5.279 <0.001 IL-10(pg/mL) 31.29(28.21~34.41) 31.28(30.03~33.84) Z=-1.370 0.171 IL-12(pg/mL) 14.66(11.78~18.06) 13.60(10.37~15.52) Z=-1.985 0.047 IL-13(pg/mL) 0.86 (0.80~0.91) 0.89 (0.75~1.04) Z=-1.234 0.217 TNF-α(pg/mL) 77.64±31.64 128.48±25.33 t=-10.177 <0.001
下载: 导出CSV
表 3 多因素Logistic回归分析SAP的影响因素
Table 3. Multivariate Logistic regression analysis of independent risk factors of SAP patients
因素 β值 SE P值 OR值 95% CI 性别 0.037 1.046 0.972 1.038 0.134~1.228 年龄 0.117 0.045 0.880 1.170 0.184~10.110 BMI -0.269 0.140 0.054 0.764 0.581~1.005 饮酒史 0.576 1.532 0.707 1.778 0.088~35.804 吸烟史 0.165 1.148 0.886 1.179 0.124~11.180 糖尿病 0.185 1.205 0.878 1.203 0.113~12.763 高血压 -0.598 1.133 0.598 0.550 0.060~5.070 GM-CSF -0.023 0.100 0.818 0.977 0.803~1.189 IFN-γ 0.174 0.071 0.014 1.190 1.036~1.367 IL-1β 0.071 0.068 0.298 1.074 0.939~1.227 IL-2 0.393 0.540 0.466 1.482 0.514~4.271 IL-4 0.042 0.061 0.493 1.043 0.925~1.175 IL-5 4.655 2.411 0.054 105.074 0.932~11 851.669 IL-6 0.138 0.036 <0.001 1.148 1.070~1.231 IL-7 -0.099 0.205 0.629 0.906 0.606~1.353 IL-8 -0.054 0.038 0.161 0.948 0.879~1.022 IL-10 0.097 0.051 0.057 1.101 0.997~1.216 IL-12 -0.099 0.111 0.373 0.906 0.729~1.126 IL-13 1.232 1.592 0.439 3.427 0.151~77.664 TNF-α 0.096 0.025 <0.001 1.100 1.048~1.155
下载: 导出CSV
-
[1] BANKS PA, BOLLEN TL, DERVENIS C, et al. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus[J]. Gut, 2013, 62(1): 102-111. DOI: 10.1136/gutjnl-2012-302779. [2] LANKISCH PG, APTE M, BANKS PA. Acute pancreatitis[J]. Lancet, 2015, 386(9988): 85-96. DOI: 10.1016/S0140-6736(14)60649-8. [3] BOXHOORN L, VOERMANS RP, BOUWENSE SA, et al. Acute pancreatitis[J]. Lancet, 2020, 396(10252): 726-734. DOI: 10.1016/S0140-6736(20)31310-6. [4] STAUBLI S M, OERTLI D, NEBIKER CA. Laboratory markers predicting severity of acute pancreatitis[J]. Crit Rev Clin Lab Sci, 2015, 52(6): 273-283. DOI: 10.3109/10408363.2015.1-051659. [5] LUO XP, WANG J, WU Q, et al. Research advances in acute pancreatitis scoring system[J]. J Clin Hepatol, 2022, 38(9): 2188-2192. DOI: 10.3969/j.issn.1001-5256.2022.09.046.罗秀平, 王洁, 吴青, 等. 急性胰腺炎评分系统的研究进展[J]. 临床肝胆病杂志, 2022, 38(9): 2188-2192. DOI: 10.3969/j.issn.1001-5256.2022.09.046. [6] KENEZ J. Charles Richet and the development of immuno-allergology[J]. Orv Hetil, 1975, 116(42): 2489-2492. DOI: 10.1016/S0140-6736(08)60107-5. [7] BHATIA M, WONG FL, CAO Y, et al. Pathophysiology of acute pancreatitis[J]. Pancreatology, 2005, 5(2-3): 132-144. DOI: 10.1159/000085265. [8] Pancreatic Surgery Group, Chinese Society of Surgery, Chinese Medical Association, Guidelines for diagnosis and treatment of acute pancreatitis in China (2021)[J]. Chin J Dig Surg, 2021, 20(7): 730-739. DOI: 10.3760/cma.j.cn112139-20210416-00172.中华医学会外科学分会胰腺外科学组. 中国急性胰腺炎诊治指南(2021)[J]. 中华消化外科杂志, 2021, 20(7): 730-739. DOI: 10.3760/cma.j.cn112139-20210416-00172. [9] ZHUANG J, ZHU WW, ZHANG C. Establishment and validation of a noninvasive diagnostic model for chronic hepatitis B liver fibrosis based on LASSO regression[J]. J Clin Hepatol, 2022, 38(8): 1790-1795. DOI: 10.3969/j.issn.1001-5256.2022.08.014.壮健, 朱韦文, 张超. 基于LASSO回归的慢性乙型肝炎肝纤维化无创诊断模型的构建及验证[J]. 临床肝胆病杂志, 2022, 38(8): 1790-1795. DOI: 10.3969/j.issn.1001-5256.2022.08.014. [10] GIBOR U, PERRY Z, NETZ U, et al. Circulating cell-free DNA in patients with acute biliary pancreatitis: association with disease markers and prolonged hospitalization time-A prospective cohort study[J]. Ann Surg, 2020, 2(3): 77-78. DOI: 10.1097/SLA.0000000000004679. [11] STERNBY H, HARTMAN H, THORLACIUS H, et al. The initial course of IL1β, IL-6, IL-8, IL-10, IL-12, IFN-γ and TNF-α with regard to severity grade in acute pancreatitis[J]. Biomolecules, 2021, 11(4). DOI: 10.3390/biom11040591. [12] AOUN E, CHEN J, REIGHARD D, et al. Diagnostic accuracy of interleukin-6 and interleuk- in-8 in predicting severe acute pancreatitis: a meta-analysis[J]. Pancreatology, 2009, 9(6): 777 -785. DOI: 10.1159/000214191. [13] LIANG ZX, PAN WC, MAI JW, et al. Application value of serum hs-CRP, IL-6 and TNF-α in the evaluation of acute pancreatitis[J]. Chin J Mod Drug Appl, 2020, 14(22): 48-50. DOI: 10.14164/j.cnki.cn11-5581/r.2020.22.021.梁灼星, 潘伟才, 麦静雯, 等. 血清hs-CRP、IL-6、TNF-α在急性胰腺炎病情评估中的应用价值研究[J]. 中国现代药物应用, 2020, 14(22): 48-50. DOI: 10.14164/j.cnki.cn11-5581/r.2020.22.021. [14] DI GIOIA M, SPREAFICO R, SPRINGSTEAD JR, et al. Endogenous oxidized phospholipids reprogram cellular metabolism and boost hyperinflammation[J]. Nat Immunol, 2020, 21(1): 42-53. DOI: 10.1038/s41590-019-0539-2. [15] YE M, JOOSSE M E, LIU L, et al. Deletion of IL-6 exacerbates colitis and induces systemic inflammation in IL-10-deficient mice[J]. J Crohns Colitis, 2020, 14(6): 831-840. DOI: 10.1093/ecco-jcc/jjz176. [16] ZHANG XP, CHEN L, HU QF, et al. Effects of large dose of dexamethasone on inflammatory mediators and pancreatic cell apoptosis of rats with severe acute pancreatitis[J]. World J Gastroenterol, 2007, 13(41): 5506-5511. DOI: 10.3748/wjg.v13.i41.5506. [17] HUANG Z, MA X, JIA X, et al. Prevention of severe acute pancreatitis with cyclooxygenase-2 inhibitors: A randomized controlled clinical trial[J]. Am J Gastroenterol, 2020, 115(3): 473-480. DOI: 10.14309/ajg.0000000000000529. [18] HE WH, ZHENG X, ZHU Y, et al. Comparison of APACHEⅡ, Ranson, BISAP and CTSI scores in early prediction of the severity of acute pancreatitis based on large sample database[J]. Chin J Pancreatol, 2019, 19(3): 172-176. DOI: 10.3760/cma.j.issn.1674-1935.2019.03.004.何文华, 郑西, 祝荫, 等. 基于大样本数据库比较APACHEⅡ、Ranson、BISAP和CTSI评分在早期预测急性胰腺炎病情严重程度的价值[J]. 中华胰腺病杂志, 2019, 19(3): 172-176. DOI: 10.3760/cma.j.issn.1674-1935.2019.03.004. -

 本文二维码
本文二维码
计量
- 文章访问数: 222
- HTML全文浏览量: 74
- PDF下载量: 44
- 被引次数: 0

