
 PDF下载 ( 706 KB)
PDF下载 ( 706 KB)

传统非侵入性纤维化模型对慢性乙型肝炎合并代谢相关脂肪性肝病发生显著肝纤维化的诊断价值
DOI: 10.3969/j.issn.1001-5256.2023.09.012
Value of traditional noninvasive fibrosis models in diagnosis of significant liver fibrosis in patients with chronic hepatitis B and metabolic associated fatty liver disease
-
摘要:
目的 评价传统非侵入性纤维化模型对慢性乙型肝炎(CHB)合并代谢相关脂肪性肝病(MAFLD)发生显著肝纤维化的诊断价值。 方法 纳入2014年9月—2020年12月在广东省中医院肝病科行肝脏病理检查且同时符合CHB和MAFLD诊断标准的患者共499例。采用Scheuer评分系统评价肝纤维化程度。呈非正态分布的计量资料组间比较采用Mann-Whitney U检验;采用Spearman对各无创诊断方法与肝脏纤维化程度进行相关性分析;绘制受试者工作特征曲线(ROC曲线),评价FibroScan、GPR、APRI、FIB-4、LPRI对CHB合并MAFLD的诊断价值;利用二元Logistic回归分析构建联合模型,将联合模型与5种指标单独应用时的ROC曲线下面积(AUC)进行比较;采用Delong检验对各无创诊断方法进行AUC的两两比较。 结果 无或轻度肝纤维化组(S0 ~ S1)198例,显著肝纤维化组(S≥2)301例。S≥2组的各项临床指标均高于S0 ~ S1组,其中ALT、AST、GGT、TBil、GPR、FIB-4、APRI、LPRI、LSM差异均有统计学意义(P值均<0.05)。Spearman相关性分析结果显示,GPR、FIB-4、APRI、LSM、LPRI与肝脏纤维化分期均呈正相关(r值分别为0.393、0.414、0.449、0.553、0.580,P值均<0.001)。ROC曲线分析显示,GPR、FIB-4、APRI、LSM、LPRI单独应用诊断显著性肝纤维化的AUC分别为0.704、0.715、0.740、0.787、0.802;利用二元Logistic回归分析构建GPR、FIB-4、APRI、LSM的联合模型LGAF,LGAF诊断显著性肝纤维化的AUC为0.814;将LGAF分别与GPR、FIB-4、APRI、LSM、LPRI的AUC进行比较,除了与LPRI相比差异无统计学意义以外,其余均有统计学意义(Z值分别为5.184、4.884、4.117、2.120,P值均<0.05)。 结论 FibroScan、GPR、APRI、FIB-4、LPRI五项数据模型对CHB合并MAFLD发生显著肝纤维化的诊断价值与CHB合并NAFLD发生显著纤维化的诊断价值相似,对于临床实际无创评估肝纤维化的应用有参考及指导价值。 Abstract:Objective To investigate the value of traditional noninvasive fibrosis models in the diagnosis of significant liver fibrosis in patients with chronic hepatitis B (CHB) and metabolic associated fatty liver disease (MAFLD). Methods A total of 499 patients who underwent liver pathological examination in Department of Hepatology, Guangdong Provincial Hospital of Traditional Chinese Medicine, from September 2014 to December 2020 and met the diagnostic criteria for CHB and MAFLD were enrolled in this study. The Scheuer scoring system was used to evaluate the degree of liver fibrosis. The Mann-Whitney U test was used for comparison of normally distributed continuous data between groups. A Spearman correlation analysis was used to investigate the correlation of each noninvasive diagnostic method with the degree of liver fibrosis; the receiver operating characteristic (ROC) curve was plotted to investigate the value of FibroScan, gamma-glutamyl transpeptidase-to-platelet ratio (GPR), aspartate aminotransferase-to-platelet ratio index (APRI), fibrosis-4 (FIB-4), and liver stiffness measurement-to-platelet ratio index (LPRI) in the diagnosis of CHB with MAFLD; a binary Logistic regression analysis was used to construct a combined model, and the area under the ROC curve (AUC) was compared between the combined model and the five indicators used alone. The DeLong method was used for comparison of AUC between any two noninvasive diagnostic methods. Results There were 198 patients in the group with no or mild liver fibrosis (S0-S1) and 301 patients in the group with significant liver fibrosis (S≥2). The S≥2 group had higher clinical indicators than the S0-S1 group, with significant differences between the two groups in alanine aminotransferase, aspartate aminotransferase, gamma-glutamyl transpeptidase, total bilirubin, GPR, FIB-4, APRI, LPRI, and liver stiffness measurement (LSM) (all P<0.05). The Spearman correlation analysis showed that GPR, FIB-4, APRI, LSM, and LPRI were positively correlated with the stage of liver fibrosis (r = 0.393, 0.414, 0.449, 0.553, and 0.580, all P<0.001). The ROC curve analysis showed that GPR, FIB-4, APRI, LSM, and LPRI used alone had an AUC of 0.704, 0.715, 0.740, 0.787, and 0.802, respectively, in the diagnosis of significant liver fibrosis. The binary Logistic regression analysis was used to construct a combined LGAF model of GPR, FIB-4, APRI, and LSM, which had an AUC of 0.814 in the diagnosis of significant liver fibrosis. LGAF was compared with GPR, FIB-4, APRI, LSM, and LPRI, respectively, in terms of AUC, and the results showed that there was a significant difference between LGAF and all five indicators except LPRI (Z=5.184, 4.884, 4.117, and 2.120, all P<0.05). Conclusion The five data models of FibroScan, GPR, APRI, FIB-4, and LPRI have a similar value in the diagnosis of significant liver fibrosis in CHB with MAFLD compared with the combined LGAF model, which provides reference and guidance for the application of noninvasive assessment of liver fibrosis in clinical practice. -
Key words:
- Hepatitis B, Chronic /
- Non-alcoholic Fatty Liver Disease /
- Hepatic Fibrosis /
- Diagnosis
-
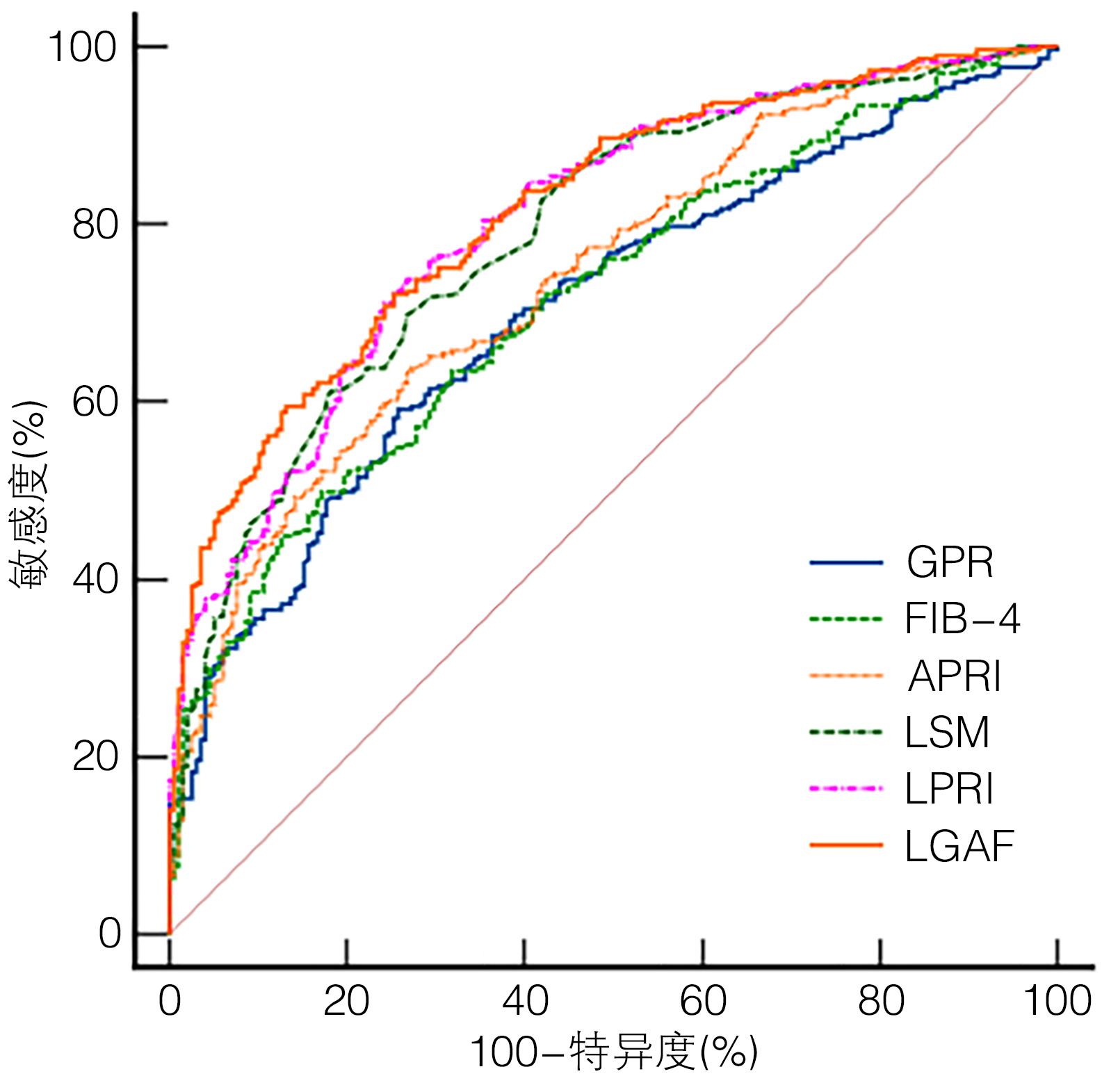
图 1 6种多参数模型单独应用及联合应用诊断S≥2的ROC曲线分析
Figure 1. Analysis of ROC curve for diagnosis of S≥2 using six multi-parameter models alone and in combination
表 1 两组间基本资料比较
Table 1. Comparison of basic data between the two groups
项目 S0 ~ S1组(n=198) S≥2组(n=301) 统计值 P值 男/女(例) 165/33 244/57 χ2=0.416 0.519 年龄(岁) 40.00(35.00 ~ 47.00) 42.00(35.00 ~ 49.00) Z=-1.636 0.102 BMI(kg/m2) 25.02(23.68 ~ 26.98) 25.20(23.71 ~ 27.17) Z=-0.137 0.891 ALT(U/L) 31.50(22.00 ~ 46.25) 40.00(26.00 ~ 72.00) Z=-4.130 <0.001 AST(U/L) 23.00(19.00 ~ 29.00) 30.00(23.00 ~ 48.50) Z=-7.316 <0.001 ALP(U/L) 69.50(59.75 ~ 81.00) 70.00(57.00 ~ 85.50) Z=-0.612 0.541 GGT(U/L) 27.50(20.75 ~ 38.25) 36.00(24.00 ~ 60.00) Z=-5.651 <0.001 TBil(mmol/L) 11.25(9.10 ~ 14.80) 12.50(9.25 ~ 16.90) Z=-2.225 0.026 GPR 0.24(0.17 ~ 0.36) 0.40(0.25 ~ 0.66) Z=-7.734 <0.001 FIB-4 0.74(0.57 ~ 1.00) 1.08(0.76 ~ 1.74) Z=-8.125 <0.001 APRI 0.27(0.19 ~ 0.35) 0.41(0.28 ~ 0.72) Z=-9.082 <0.001 LPRI 2.46(1.90 ~ 3.09) 4.03(2.94 ~ 6.88) Z=-11.434 <0.001 LSM 5.35(4.40 ~ 6.80) 7.90(6.20 ~ 11.70) Z=-10.859 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 各无创诊断方法与肝脏纤维化程度的相关性分析
Table 2. Spearman between various non-invasive diagnostic methods and the degree of liver fibrosis
指标 r值 95%CI P值 GPR 0.393 0.322 ~ 0.467 <0.001 FIB-4 0.414 0.339 ~ 0.487 <0.001 APRI 0.449 0.378 ~ 0.516 <0.001 LSM 0.553 0.484 ~ 0.623 <0.001 LPRI 0.580 0.513 ~ 0.644 <0.001
下载: 导出CSV
表 3 LSM、GPR、APRI、FIB-4单独应用及联合应用对S≥2诊断价值的比较
Table 3. Comparison of diagnostic value of LSM, GPR, APRI and FIB-4 alone and in combination for S≥2
指标 临界值 AUC(95%CI) 敏感度 (%) 特异度 (%) 阳性预测值 (%) 阴性预测值 (%) P值 GPR 0.314 0.704(0.662 ~ 0.744) 59.14 74.24 77.70 54.40 <0.001 FIB-4 1.093 0.715(0.673 ~ 0.754) 49.83 82.83 81.50 52.10 <0.001 APRI 0.339 0.740(0.699 ~ 0.778) 63.46 73.23 78.30 56.90 <0.001 LSM 6.600 0.787(0.749 ~ 0.822) 69.77 73.23 79.80 61.40 <0.001 LPRI 3.030 0.802(0.765 ~ 0.836) 73.40 74.70 81.00 64.60 <0.001 LGAF1) 0.525 0.814(0.777 ~ 0.848) 72.09 74.75 81.30 63.80 <0.001 注: 1)LGAF=LSM+GPR+APRI+FIB-4。
下载: 导出CSV
-
[1] WANG CE, XU WT, GONG J, et al. Treatment of patients with nonalcoholic fatty liver disease[J]. Clin J Med Offic, 2022, 50( 9): 897- 899, 903. DOI: 10.16680/j.1671-3826.2022.09.06.王彩娥, 许文涛, 宫建, 等. 非酒精性脂肪性肝病治疗研究进展[J]. 临床军医杂志, 2022, 50( 9): 897- 899, 903. DOI: 10.16680/j.1671-3826.2022.09.06. [2] FARRELL GC, WONG VW, CHITTURI S. NAFLD in Asia—as common and important as in the West[J]. Nat Rev Gastroenterol Hepatol, 2013, 10( 5): 307- 318. DOI: 10.1038/nrgastro.2013.34. [3] MAK LY, SETO WK, HUI RW, et al. Fibrosis evolution in chronic hepatitis B e antigen-negative patients across a 10-year interval[J]. J Viral Hepat, 2019, 26( 7): 818- 827. DOI: 10.1111/jvh.13095. [4] ESLAM M, SANYAL AJ, GEORGE J, et al. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease[J]. Gastroenterology, 2020, 158( 7): 1999- 2014. DOI: 10.1053/j.gastro.2019.11.312. [5] GONG H, LI LP. Value of Fibroscan combined with GPR, APRI, NFS or FIB-4 for progressive liver fibrosis in patients with chronic hepatitis B and nonalcoholic fatty liver disease[J]. J Clin Hepatol, 2020, 36( 3): 541- 545. DOI: 10.3969/j.issn.1001-5256.2020.03.014.龚航, 李良平. FibroScan分别与GPR、APRI、NFS、FIB-4联合应用对慢性乙型肝炎合并非酒精性脂肪性肝病进展期肝纤维化的诊断价值比较[J]. 临床肝胆病杂志, 2020, 36( 3): 541- 545. DOI: 10.3969/j.issn.1001-5256.2020.03.014. [6] WANG Q, XIE W, LIU L, et al. Serum markers for predicting advanced fibrosis in patients with chronic hepatitis B and nonalcoholic fatty liver disease[J]. Medicine(Baltimore), 2021, 100( 18): e25327. DOI: 10.1097/MD.0000000000025327. [7] Foundation for Hepatitis Prevention and Control; Chinese Society of Infectious Disease and Chinese Society of Hepatology, Chinese Medical Association; Liver Disease Committee of Chinese Research Hospital Association. Consensus on clinical application of transient elastography detecting liver fibrosis: a 2018 update[J]. Chin J Hepatol, 2019, 27( 3): 182- 191. DOI: 10.3760/cma.j.issn.1007-3418.2019.03.004.中国肝炎防治基金会, 中华医学会感染病学分会, 中华医学会肝病学分会和中国研究型医院学会肝病专业委员会. 瞬时弹性成像技术诊断肝纤维化专家共识(2018年更新版)[J]. 中华肝脏病杂志, 2019, 27( 3): 182- 191. DOI: 10.3760/cma.j.issn.1007-3418.2019.03.004. [8] CHENG DY, LI B, JI SB, et al. Application of transient elastography in noninvasive diagnosis of liver fibrosis[J/CD]. Chin J Liver Dis(Electronic Version), 2021, 13( 4): 9- 13. DOI: 10.3969/j.issn.1674-7380.2021.04.003.程丹颖, 李贲, 纪世博, 等. 瞬时弹性成像技术在肝纤维化无创诊断中的应用[J/CD]. 中国肝脏病杂志(电子版), 2021, 13( 4): 9- 13. DOI: 10.3969/j.issn.1674-7380.2021.04.003. [9] PARK JJ, PARK JY, KIM DY, et al. Prediction of significant fibrosis in chronic hepatitis C patients with normal ALT[J]. Hepatogastroenterology, 2011, 58( 109): 1321- 1327. DOI: 10.5754/hge11041. [10] OKAJIMA A, SUMIDA Y, TAKETANI H, et al. Liver stiffness measurement to platelet ratio index predicts the stage of liver fibrosis in non-alcoholic fatty liver disease[J]. Hepatol Res, 2017, 47( 8): 721- 730. DOI: 10.1111/hepr.12793. [11] Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B(version 2019)[J]. J Clin Hepatol, 2019, 35( 12): 2648- 2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35( 12): 2648- 2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [12] ESLAM M, SARIN SK, WONG VW, et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease[J]. Hepatol Int, 2020, 14( 6): 889- 919. DOI: 10.1007/s12072-020-10094-2. [13] GOODMAN ZD. Grading and staging systems for inflammation and fibrosis in chronic liver diseases[J]. J Hepatol, 2007, 47( 4): 598- 607. DOI: 10.1016/j.jhep.2007.07.006. [14] Chinese Society of Hepatology, Chinese Medical Association; Chinese Society of Gastroenterology, Chinese Medical Association; Chinese Society of Infectious Diseases, Chinese Medical Association. Consensus on the diagnosis and therapy of hepatic fibrosis(2019)[J]. J Clin Hepatol, 2019, 35( 10): 2163- 2172. DOI: 10.3969/j.issn.1001-5256.2019.10.007.中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会感染病学分会. 肝纤维化诊断及治疗共识(2019年)[J]. 临床肝胆病杂志, 2019, 35( 10): 2163- 2172. DOI: 10.3969/j.issn.1001-5256.2019.10.007. [15] LEMOINE M, SHIMAKAWA Y, NAYAGAM S, et al. The gamma-glutamyl transpeptidase to platelet ratio(GPR) predicts significant liver fibrosis and cirrhosis in patients with chronic HBV infection in West Africa[J]. Gut, 2016, 65( 8): 1369- 1376. DOI: 10.1136/gutjnl-2015-309260. [16] LIN S, HUANG J, WANG M, et al. Comparison of MAFLD and NAFLD diagnostic criteria in real world[J]. Liver Int, 2020, 40( 9): 2082- 2089. DOI: 10.1111/liv.14548. [17] YAMAMURA S, ESLAM M, KAWAGUCHI T, et al. MAFLD identifies patients with significant hepatic fibrosis better than NAFLD[J]. Liver Int, 2020, 40( 12): 3018- 3030. DOI: 10.1111/liv.14675. [18] van KLEEF LA, CHOI H, BROUWER WP, et al. Metabolic dysfunction-associated fatty liver disease increases risk of adverse outcomes in patients with chronic hepatitis B[J]. JHEP Rep, 2021, 3( 5): 100350. DOI: 10.1016/j.jhepr.2021.100350. [19] RUGIVARODOM M, PONGPAIBUL A, CHAINUVATI S, et al. Prognostic relevance of metabolic dysfunction-associated steatohepatitis for patients with chronic hepatitis B[J]. J Clin Transl Hepatol, 2023, 11( 1): 76- 87. DOI: 10.14218/JCTH.2022.00055. [20] DONG M, WU J, YU X, et al. Validation and comparison of seventeen noninvasive models for evaluating liver fibrosis in Chinese hepatitis B patients[J]. Liver Int, 2018, 38( 9): 1562- 1570. DOI: 10.1111/liv.13688. [21] EDDOWES PJ, SASSO M, ALLISON M, et al. Accuracy of fibroscan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease[J]. Gastroenterology, 2019, 156( 6): 1717- 1730. DOI: 10.1053/j.gastro.2019.01.042. [22] RIGOR J, DIEGUES A, PRESA J, et al. Noninvasive fibrosis tools in NAFLD: validation of APRI, BARD, FIB-4, NAFLD fibrosis score, and Hepamet fibrosis score in a Portuguese population[J]. Postgrad Med, 2022, 134( 4): 435- 440. DOI: 10.1080/00325481.2022.2058285. [23] HUANG CM, HU ZW, NIE YQ, et al. The value of non-invasive diagnostic model in predicting liver fibrosis in patients with chronic hepatitis B combined with non-alcoholic fatty liver disease[J]. Chin J Gastroenter Hepatol, 2019, 28( 8): 915- 918. DOI: 10.3969/j.issn.1006-5709.2019.08.018.黄春明, 胡中伟, 聂玉强, 等. 无创诊断模式预测慢性乙型肝炎合并非酒精性脂肪肝患者肝纤维化的价值[J]. 胃肠病学和肝病学杂志, 2019, 28( 8): 915- 918. DOI: 10.3969/j.issn.1006-5709.2019.08.018. [24] CHEN X, GOH GB, HUANG J, et al. Validation of non-invasive fibrosis scores for predicting advanced fibrosis in metabolic-associated fatty liver disease[J]. J Clin Transl Hepatol, 2022, 10( 4): 589- 594. DOI: 10.14218/JCTH.2021.00311. [25] UCAR F, SEZER S, GINIS Z, et al. APRI, the FIB-4 score, and Forn's index have noninvasive diagnostic value for liver fibrosis in patients with chronic hepatitis B[J]. Eur J Gastroenterol Hepatol, 2013, 25( 9): 1076- 1081. DOI: 10.1097/MEG.0b013e32835fd699. [26] XIAO G, YANG J, YAN L. Comparison of diagnostic accuracy of aspartate aminotransferase to platelet ratio index and fibrosis-4 index for detecting liver fibrosis in adult patients with chronic hepatitis B virus infection: a systemic review and meta-analysis[J]. Hepatology, 2015, 61( 1): 292- 302. DOI: 10.1002/hep.27382. [27] ZHANG Z, WANG G, KANG K, et al. The diagnostic accuracy and clinical utility of three noninvasive models for predicting liver fibrosis in patients with HBV infection[J]. PLoS One, 2016, 11( 4): e0152757. DOI: 10.1371/journal.pone.0152757. [28] LI Q, SONG J, HUANG Y, et al. The gamma-glutamyl-transpeptidase to platelet ratio does not show advantages than APRI and Fib-4 in diagnosing significant fibrosis and cirrhosis in patients with chronic hepatitis B: A retrospective cohort study in China[J]. Medicine(Baltimore), 2016, 95( 16): e3372. DOI: 10.1097/MD.0000000000003372. [29] REN T, WANG H, WU R, et al. Gamma-glutamyl transpeptidase-to-platelet ratio predicts significant liver fibrosis of chronic hepatitis B patients in China[J]. Gastroenterol Res Pract, 2017, 2017: 7089702. DOI: 10.1155/2017/7089702. [30] LUO J, DU Z, LIANG D, et al. Gamma-Glutamyl Transpeptidase-to-Platelet ratio predicts liver fibrosis in patients with concomitant chronic hepatitis B and nonalcoholic fatty liver disease[J]. J Clin Lab Anal, 2022, 36( 8): e24596. DOI: 10.1002/jcla.24596. [31] HUANG CM, YANG Z, NIE YQ, et al. Prediction of liver fibrosis by gamma-glutamyl-transpeptidase-to-platelet ratio in patients with chronic hepatitis B viral infection with normal serum transaminase levels[J]. J Prac Hepatol, 2018, 21( 6): 859- 862. DOI: 10.3969/j.issn.1672-5069.2018.06.009.黄春明, 杨湛, 聂玉强, 等. γ-谷氨酰转肽酶/血小板比值对血清转氨酶正常的慢性HBV感染者肝纤维化的预测价值分析[J]. 实用肝脏病杂志, 2018, 21( 6): 859- 862. DOI: 10.3969/j.issn.1672-5069.2018.06.009. [32] European Association for the Study of the Liver. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection[J]. J Hepatol, 2017, 67( 2): 370- 398. DOI: 10.1016/j.jhep.2017.03.021. [33] Korean Association for the Study of the Liver(KASL). KASL clinical practice guidelines for management of chronic hepatitis B[J]. Clin Mol Hepatol, 2022, 28( 2): 276- 331. DOI: 10.3350/cmh.2022.0084. [34] TERRAULT NA, LOK A, MCMAHON BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance[J]. Hepatology, 2018, 67( 4): 1560- 1599. DOI: 10.1002/hep.29800. [35] ZHANG GL, XU SC, ZENG J, et al. Optimizing the use of the gamma-glutamyl transpeptidase-to-platelet ratio and transient elastography to identify liver cirrhosis in patients with chronic hepatitis B concurrent with nonalcoholic fatty liver disease[J]. Dis Markers, 2019, 2019: 2585409. DOI: 10.1155/2019/2585409. [36] LI Q, HUANG C, XU W, et al. Accuracy of FibroScan in analysis of liver fibrosis in patients with concomitant chronic hepatitis B and nonalcoholic fatty liver disease[J]. Medicine(Baltimore), 2020, 99( 23): e20616. DOI: 10.1097/MD.0000000000020616. [37] ZHOU JL, WANG BQ, SUN YM, et al. Application value of liver stiffness measurement-to-platelet ratio index score in diagnosis of hepatitis B liver fibrosis and liver cirrhosis[J]. J Clin Hepatol, 2022, 38( 7): 1529- 1533. DOI: 10.3969/j. issn. 1001-5256.2022.07.014.周家玲, 王冰琼, 孙亚朦, 等. LPRI评分在乙型肝炎肝纤维化及肝硬化中的诊断价值[J]. 临床肝胆病杂志, 2022, 38( 7): 1529- 1533. DOI: 10.3969/j.issn.1001-5256.2022.07.014. -

 本文二维码
本文二维码
计量
- 文章访问数: 446
- HTML全文浏览量: 114
- PDF下载量: 50
- 被引次数: 0

