
 PDF下载 ( 901 KB)
PDF下载 ( 901 KB)

慢加急性肝衰竭:基于起病表现的新型临床分型特征及预后分析
DOI: 10.3969/j.issn.1001-5256.2023.10.015
Acute-on-chronic liver failure: Features and prognosis of a new clinical classification system based on onset manifestations
-
摘要:
目的 分析慢加急性肝衰竭(ACLF)起病时肝内、外器官衰竭特点,探索新型ACLF临床分型特征,为疾病诊治及转归提供依据。 方法 回顾性收集2015年1月—2022年10月于首都医科大学附属北京佑安医院住院治疗的首次确诊为ACLF患者的临床资料。根据起病时肝内、外器官衰竭的情况,将患者分为Ⅰ型和Ⅱ型ACLF。Ⅰ型ACLF为慢性肝病基础上的肝功能衰竭;Ⅱ型ACLF为慢性肝病急性失代偿合并多脏器功能衰竭。分析Ⅰ型和Ⅱ型ACLF患者的临床特征,采用受试者工作特征曲线(ROC曲线)评估MELD、MELD-Na和CLIF-C ACLF评分系统对Ⅰ型和Ⅱ型ACLF患者90天预后的预测价值。符合正态分布的计量资料两组间比较采用成组t检验;非正态分布的计量资料两组间比较采用Wilcoxon秩和检验;计数资料两组间比较采用χ2检验或Fisher精确检验。 结果 共纳入582例ACLF患者,其中Ⅰ型ACLF患者535例,Ⅱ型ACLF患者47例。两组患者的病因均以乙型肝炎和酒精性肝病为主,组间差异均无统计学意义(P值均>0.05)。Ⅰ型ACLF以慢性非肝硬化肝病(28.2%)和代偿性肝硬化(56.8%)为主,Ⅱ型ACLF以代偿性肝硬化(34.0%)和失代偿性肝硬化(61.7%)为主,Ⅰ型和Ⅱ型ACLF患者的肝病基础差异有统计学意义(P<0.001)。Ⅱ型ACLF患者的中位MELD评分、MELD-Na评分和CLIF-C ACLF评分高于Ⅰ型,差异均有统计学意义(P值均<0.001)。Ⅱ型ACLF患者28天和90天病死率分别为38.3%和53.2%,高于Ⅰ型患者的15.5%和27.5%,差异均有统计学意义(P值均<0.001)。对于病程中未进展至多脏器衰竭的Ⅰ型ACLF患者,死亡组MELD评分升高者占63.7%,存活组MELD升高者占10.1%,差异有统计学意义(P<0.001);但是对病情进展至多脏器衰竭的Ⅰ型ACLF患者,在存活组、死亡组间MELD评分变化趋势差异无统计学意义(P>0.05)。在Ⅰ型ACLF患者中,MELD评分、MELD-Na评分和CLIF-C ACLF评分的ROC曲线下面积(AUC)分别为0.735、0.737和0.740,两两比较差异均无统计学意义(P值均>0.05)。在Ⅱ型ACLF患者中,CLIF-C ACLF评分的AUC为0.880,高于MELD评分(AUC=0.560)和MELD-Na评分(AUC=0.513),差异均有统计学意义(P值均<0.01)。 结论 Ⅰ型ACLF与Ⅱ型ACLF的肝病基础、临床特征和预后均存在差异,预后评分系统侧重不同,为新型ACLF临床分型提供了循证医学依据。 Abstract:Objective To investigate the characteristics of intrahepatic and extrahepatic organ failure at the onset of acute-on-chronic liver failure(ACLF), to explore the features of a new clinical classification system of ACLF, and to provide a basis for the diagnosis, treatment, prognostic analysis of the disease. Methods A retrospective analysis was performed for the clinical data of the patients who were hospitalized Beijing YouAn Hospital, Capital Medical University, from January 2015 to October 2022 and were diagnosed with ACLF for the first time. According to the conditions of intrahepatic and extrahepatic organ failure at disease onset, they were classified into type Ⅰ ACLF and type Ⅱ ACLF. Type Ⅰ ACLF referred to liver failure on the basis of chronic liver diseases, and type Ⅱ ACLF referred to acute decompensation of chronic liver diseases combined with multiple organ failure. The clinical features of patients with type Ⅰ or type Ⅱ ACLF were analyzed, and the receiver operating characteristic (ROC) curve was used to assess the value of MELD, MELD-Na, and CLIF-C ACLF scoring system in predicting the 90-day prognosis of ACLF patients with type Ⅰ or type Ⅱ ACLF. The independent-samples t test was used for comparison of normally distributed continuous data between two groups, and the Wilcoxon rank-sum test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test or the Fisher’s exact test was used for comparison of categorical data between two groups. Results A total of 582 patients with ACLF were enrolled, among whom there were 535 patients with type Ⅰ ACLF and 47 patients with type Ⅱ ACLF. Hepatitis B and alcoholic liver disease were the main causes in both groups, with no significant difference between the two groups (P>0.05). Chronic non-cirrhotic liver disease (28.2%) and compensated liver cirrhosis (56.8%) were the main underlying liver diseases in type Ⅰ ACLF, while compensated liver cirrhosis (34.0%) and decompensated liver cirrhosis (61.7%) were the main underlying liver diseases in type Ⅱ ACLF, and there was no significant difference in underlying liver diseases between the patients with type Ⅰ ACLF and those with type Ⅱ ACLF (P<0.001). The patients with type Ⅱ ACLF had significantly higher median MELD score, MELD-Na score, and CLIF-C ACLF score than those with type Ⅰ ACLF (all P<0.001). The patients with type Ⅱ ACLF had significantly higher 28- and 90-day mortality rates than those with type Ⅰ ACLF (38.3%/53.2% vs 15.5%/27.5%, P<0.001). For the patients with type Ⅰ ACLF who did not progress to multiple organ failure, the patients with an increase in MELD score accounted for 63.7% in the death group and 10.1% in the survival group (P<0.001), while for the patients with type Ⅰ ACLF who progressed to multiple organ failure, there was no significant difference in the change in MELD score between the survival group and the death group (P>0.05). In the patients with type Ⅰ ACLF, MELD score, MELD-Na score, and CLIF-C ACLF score had an area under the ROC curve (AUC) of 0.735, 0.737, and 0.740, respectively, with no significant difference between any two scores (all P>0.05). In the patients with type Ⅱ ACLF, CLIF-C ACLF score had a significantly higher AUC than MELD score (0.880 vs 0.560, P<0.01) and MELD-Na score (0.880 vs 0.513, P<0.01). Conclusion There are differences in underlying liver diseases, clinical features, and prognosis between type Ⅰ and type Ⅱ ACLF, and different prognosis scoring systems have different emphases, which provide a basis for the new clinical classification system of ACLF from the perspective of evidence-based medicine. -
Key words:
- Acute-On-Chronic Liver Failure /
- Disease Attributes /
- Prognosis
-
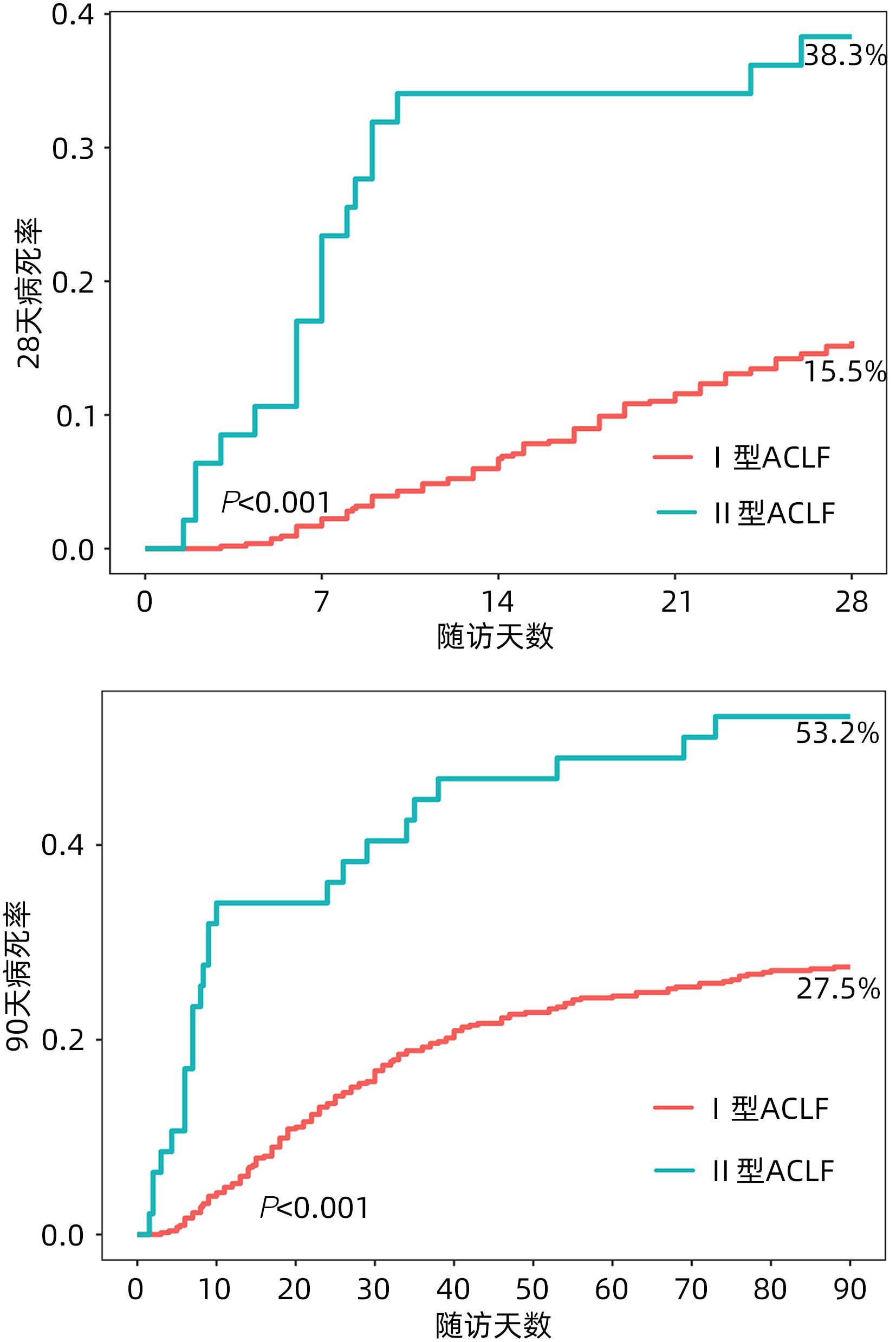
图 1 Ⅰ型和Ⅱ型ACLF患者28天和90天的累积病死率曲线
Figure 1. Cumulative incidence of 28-day and 90-day death for type Ⅰ and type Ⅱ ACLF patients
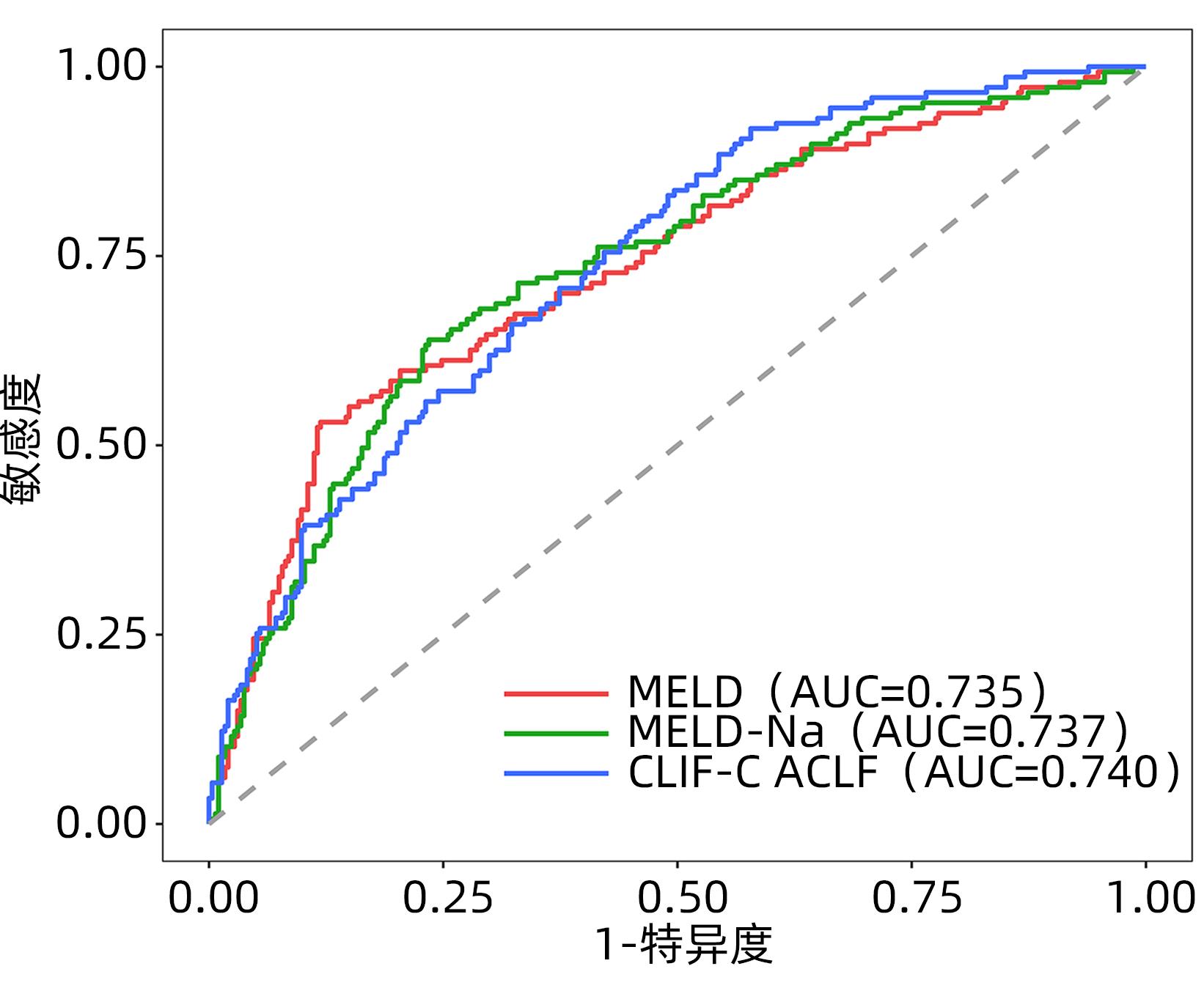
图 2 三种评分系统预测Ⅰ型ACLF患者90天病死率的ROC曲线
Figure 2. ROC curve of three scoring systems predicting 90-day mortality in patients with type Ⅰ ACLF
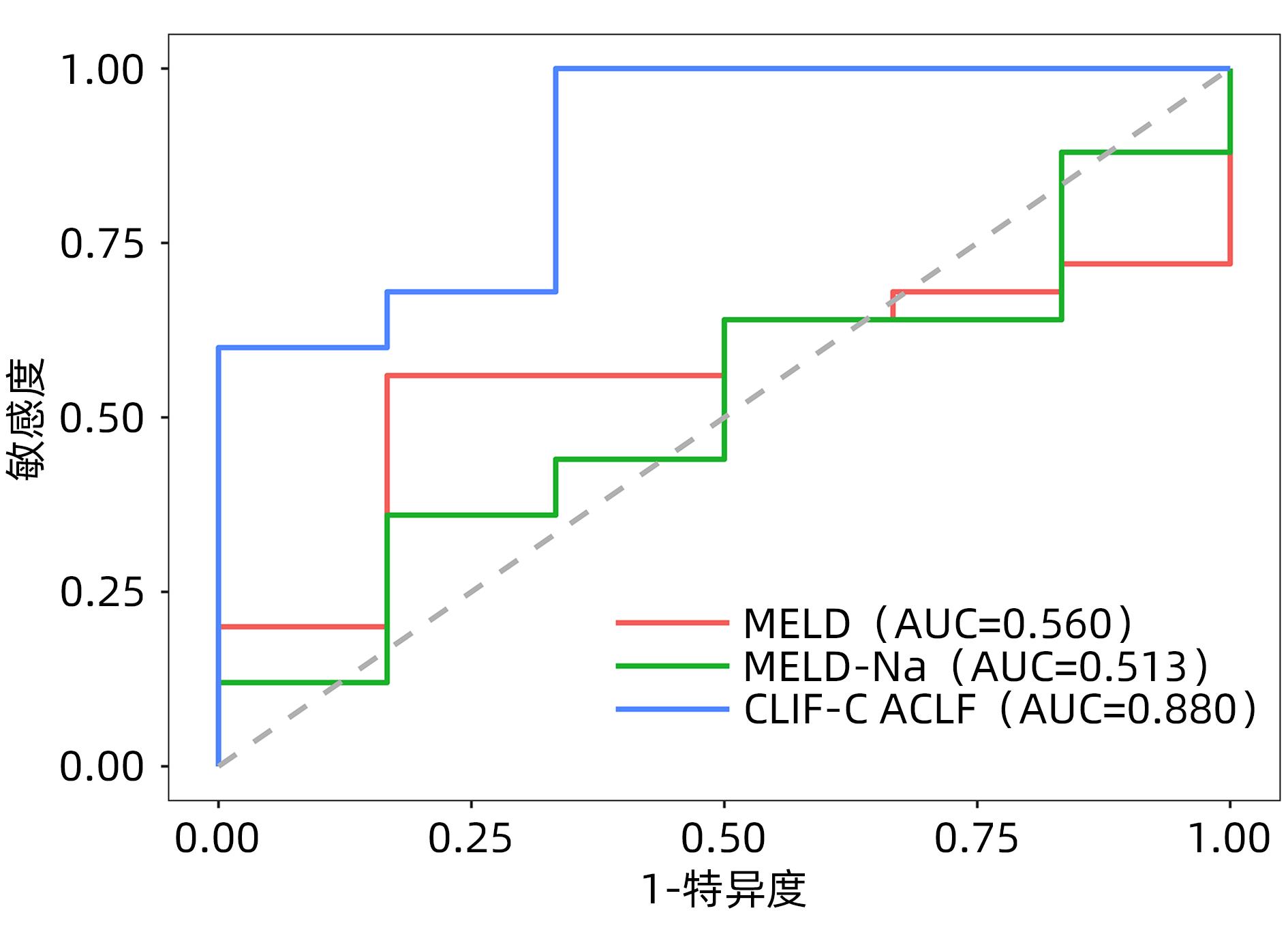
图 3 三种评分系统预测Ⅱ型ACLF患者90天病死率的ROC曲线
Figure 3. ROC curve of three scoring systems predicting 90-day mortality in patients with type Ⅱ ACLF

图 4 MELD评分的动态变化对Ⅰ型ACLF患者预后的影响
Figure 4. Influence of dynamic change of MELD score on prognosis of patients with type Ⅰ ACLF
表 1 Ⅰ型和Ⅱ型ACLF患者基线特征与预后比较
Table 1. Baseline characteristics and prognosis of patients with type Ⅰ and type Ⅱ ACLF
指标 总病例数 (n=582) Ⅰ型ACLF (n=535) Ⅱ型ACLF (n=47) 统计值 P值 男性[例(%)] 483(83.0) 440(82.2) 43(91.5) χ2=2.617 0.106 年龄(岁) 47.0(38.0~54.0) 47.0(38.0~54.0) 43.0(37.0~52.5) Z=-0.962 0.336 肝病基础[例(%)] χ2=63.935 <0.001 慢性非肝硬化肝病 153(26.3) 151(28.2) 2(4.3) χ2=11.602 0.001 代偿性肝硬化 320(55.0) 304(56.8) 16(34.0) χ2=9.058 0.003 失代偿性肝硬化 109(18.7) 80(15.0) 29(61.7) χ2=62.034 <0.001 病因[例(%)] χ2=3.320 0.708 乙型肝炎 339(58.20) 312(58.30) 27(57.40) χ2=0.013 0.908 酒精性肝病 135(23.20) 121(22.60) 14(29.80) χ2=1.247 0.264 自身免疫性肝炎 6(1.03) 5(0.93) 1(2.13) χ2=0.001 0.981 原发性胆汁性胆管炎 14(2.41) 14(2.62) 0(0.00) 0.618 乙型肝炎+酒精性肝病 48(8.25) 45(8.41) 3(6.38) χ2=0.043 0.835 药物性肝损伤 27(4.64) 26(4.86) 1(2.13) χ2=0.242 0.623 其他 13(2.23) 12(2.24) 1(2.13) χ2=0.000 >0.05 合并症[例(%)] 感染 463(93.0) 420(92.9) 43(93.5) χ2=0.020 >0.05 近期上消化道出血 48(9.3) 39(8.3) 9(19.6) χ2=6.305 0.012 肝性脑病 160(27.5) 131(24.5) 29(61.7) χ2=30.020 <0.001 腹水 467(80.2) 425(79.4) 42(89.4) χ2=2.683 0.101 ALT(U/L) 128.0(47.0~450.0) 138.0(49.0~464.0) 74.0(41.5~181.0) Z=-2.272 0.023 AST(U/L) 152.0(88.0~388.0) 154.0(91.0~403.0) 110.0(84.4~223.0) Z=-1.909 0.056 总蛋白(g/L) 62.3(56.6~68.1) 62.7(57.0~68.5) 56.2(51.2~61.2) Z=-4.485 <0.001 白蛋白(g/L) 29.3(26.3~32.5) 29.5(26.5~32.7) 27.3(24.1~31.0) Z=-2.264 0.024 总胆红素(mmol/L) 359(235~472) 352(230~465) 443(325~604) Z=-3.739 <0.001 直接胆红素(mmol/L) 241(154~333) 235(150~328) 312(218~389) Z=-3.198 0.001 凝血酶原活动度(%) 33.0(24.0~40.8) 33.0(25.0~41.0) 25.0(14.5~33.5) Z=-4.463 <0.001 国际标准化比值 2.29(1.93~2.98) 2.25(1.90~2.89) 2.79(2.23~4.80) Z=-4.551 <0.001 血尿素氮(mmol/L) 4.64(3.40~6.83) 4.52(3.37~6.43) 8.91(4.96~17.50) Z=-5.440 <0.001 血肌酐(mmol/L) 60.0(49.7~77.0) 59.0(49.0~74.2) 126.0(59.5~238.0) Z=-5.452 <0.001 血钠(mmol/L) 136(132~138) 136(132~138) 135(127~138) Z=-1.677 0.094 血钾(mmol/L) 3.86(3.45~4.21) 3.86(3.45~4.21) 3.89(3.38~4.19) Z=-0.058 0.954 血红蛋白(g/L) 118.0(98.0~136.0) 120.0(100.0~136.0) 100.0(79.5~124.0) Z=-3.886 <0.001 白细胞计数(×109/L) 6.76(4.97~9.73) 6.57(4.93~9.41) 9.43(5.72~14.80) Z=-3.693 <0.001 中性粒细胞比例(%) 71.8(63.4~79.6) 71.0(62.7~78.8) 82.0(71.3~87.8) Z=-5.101 <0.001 淋巴细胞比例(%) 16.6(10.5~23.9) 17.3(11.2~24.4) 10.6(5.0~13.3) Z=-5.624 <0.001 血小板计数(×109/L) 95.0(60.0~142.0) 97.0(62.0~144.0) 70.0(45.0~108.0) Z=-3.012 0.003 衰竭类型[例(%)] 肾衰竭 24(4.1) 0(0.0) 24(51.1) <0.001 脑衰竭 19(3.3) 0(0.0) 19(40.4) <0.001 呼吸衰竭 16(2.8) 0(0.0) 16(34.0) <0.001 循环衰竭 6(1.0) 0(0.0) 6(12.8) <0.001 凝血衰竭 237(40.7) 208(38.9) 29(61.7) χ2=9.323 0.002 疾病严重程度评分 MELD 23.0(18.6~27.5) 22.5(18.4~26.7) 31.5(26.7~39.6) Z=-7.153 <0.001 MELD-Na 24.7(20.1~31.2) 24.3(19.9~30.1) 35.2(28.6~50.0) Z=-6.709 <0.001 CLIF-C ACLF 41.7(36.8~46.4) 40.9(36.2~45.5) 51.9(48.4~55.6) Z=-9.273 <0.001 28天生存状况[例(%)] χ2=24.034 <0.001 存活 393(67.5) 376(70.3) 17(36.2) χ2=22.924 <0.001 死亡 101(17.4) 83(15.5) 18(38.3) χ2=15.637 <0.001 肝移植 88(15.1) 76(14.2) 12(25.5) χ2=4.319 0.038 90天生存状况[例(%)] χ2=30.787 <0.001 存活 300(51.5) 294(55.0) 6(12.8) χ2=28.795 <0.001 死亡 172(29.6) 147(27.5) 25(53.2) χ2=13.722 <0.001 肝移植 110(18.9) 94(17.6) 16(34.0) χ2=7.648 0.006  下载: 导出CSV
下载: 导出CSV
表 2 三种评分系统对Ⅰ型和Ⅱ型ACLF患者90天预后的预测效能
Table 2. Performance of three scoring systems in predicting 90-day prognosis in patients with type Ⅰ and type Ⅱ ACLF
评分系统 最佳临界值 AUC(95%CI) 敏感度(%) 特异度(%) Ⅰ型ACLF MELD 25.3 0.735(0.684~0.786) 53.1 88.1 MELD-Na 25.3 0.737(0.687~0.787) 63.9 76.5 CLIF-C ACLF 38.7 0.740(0.693~0.788) 83.0 51.0 Ⅱ型ACLF MELD 31.8 0.560(0.340~0.780) 83.3 56.0 MELD-Na 32.1 0.513(0.262~0.765) 83.3 36.0 CLIF-C ACLF 44.7 0.880(0.726~1.034) 100.0 66.7
下载: 导出CSV
-
[1] Liver Failure and Artificial Liver Group, Chinese Society of Infectious Diseases, Chinese Medical Association; Severe Liver Disease and Artificial Liver Group, Chinese Society of Hepatology, Chinese Medical Association. Guideline for diagnosis and treatment of liver failure(2018)[J]. J Clin Hepatol, 2019, 35( 1): 38- 44. DOI: 10.3969/j.issn.1001-5256.2019.01.007.中华医学会感染病学分会肝衰竭与人工肝学组, 中华医学会肝病学分会重型肝病与人工肝学组. 肝衰竭诊治指南(2018年版)[J]. 临床肝胆病杂志, 2019, 35( 1): 38- 44. DOI: 10.3969/j.issn.1001-5256.2019.01.007. [2] ZHANG YZ, CHEN Y. Heterogeneity of definition, clinical characteristics, treatment and prognosis of acute liver failure with chronic exacerbation[J]. Chin Hepatol, 2021, 26( 10): 1072- 1074. DOI: 10.14000/j.cnki.issn.1008-1704.2021.10.003.张译之, 陈煜. 慢加急性肝衰竭定义、临床特征、治疗与预后的异质性探讨[J]. 肝脏, 2021, 26( 10): 1072- 1074. DOI: 10.14000/j.cnki.issn.1008-1704.2021.10.003. [3] BI ZH, WANG LX, LIAN JQ. Definition, prognostic assessment, and advances in the diagnosis and treatment of acute-on-chronic liver failure[J]. J Clin Hepatol, 2022, 38( 7): 1671- 1676. DOI: 10.3969/j.issn.1001-5256.2022.07.041.毕占虎, 王临旭, 连建奇. 慢加急性肝衰竭的定义、预后评估及诊治进展[J]. 临床肝胆病杂志, 2022, 38( 7): 1671- 1676. DOI: 10.3969/j.issn.1001-5256.2022.07.041. [4] SARIN SK, CHOUDHURY A, SHARMA MK, et al. Acute-on-chronic liver failure: Consensus recommendations of the Asian Pacific association for the study of the liver(APASL): An update[J]. Hepatol Int, 2019, 13( 4): 353- 390. DOI: 10.1007/s12072-019-09946-3. [5] MOREAU R, JALAN R, GINES P, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis[J]. Gastroenterology, 2013, 144( 7): 1426- 1437.e 9. DOI: 10.1053/j.gastro.2013.02.042. [6] O’LEARY JG, REDDY KR, GARCIA-TSAO G, et al. NACSELD acute-on-chronic liver failure(NACSELD-ACLF) score predicts 30-day survival in hospitalized patients with cirrhosis[J]. Hepatology, 2018, 67( 6): 2367- 2374. DOI: 10.1002/hep.29773. [7] XU MM, YU PF, CHEN Y, et al. Amencan college of gas⁃troenterology clinical guidelines for acute-on-chromc liver failure[J]. Chin J Hepatol, 2022, 30( 2): 199- 203. DOI: 10.3760/cma.j.cn501113-20220126-00047.徐曼曼, 余朋飞, 陈煜, 等. 美国胃肠病学会《慢加急性肝衰竭临床指南》摘译[J]. 中华肝脏病杂志, 2022, 30( 2): 199- 203. DOI: 10.3760/cma. j. cn501113-20220126-00047. [8] BAJAJ JS, O’LEARY JG, LAI JC, et al. Acute-on-chronic liver failure clinical guidelines[J]. Am J Gastroenterol, 2022, 117( 2): 225- 252. DOI: 10.14309/ajg.0000000000001595. [9] MEZZANO G, JUANOLA A, CARDENAS A, et al. Global burden of disease: Acute-on-chronic liver failure, a systematic review and meta-analysis[J]. Gut, 2022, 71( 1): 148- 155. DOI: 10.1136/gutjnl-2020-322161. [10] MALINCHOC M, KAMATH PS, GORDON FD, et al. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts[J]. Hepatology, 2000, 31( 4): 864- 871. DOI: 10.1053/he.2000.5852. [11] BIGGINS SW, KIM WR, TERRAULT NA, et al. Evidence-based incorporation of serum sodium concentration into MELD[J]. Gastroenterology, 2006, 130( 6): 1652- 1660. DOI: 10.1053/j.gastro.2006.02.010. [12] JALAN R, SALIBA F, PAVESI M, et al. Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failure[J]. J Hepatol, 2014, 61( 5): 1038- 1047. DOI: 10.1016/j.jhep.2014.06.012. [13] HERNAEZ R, LIU Y, KRAMER JR, et al. Model for end-stage liver disease-sodium underestimates 90-day mortality risk in patients with acute-on-chronic liver failure[J]. J Hepatol, 2020, 73( 6): 1425- 1433. DOI: 10.1016/j.jhep.2020.06.005. [14] BAROSA R, ROQUE RAMOS L, PATITA M, et al. CLIF-C ACLF score is a better mortality predictor than MELD, MELD-Na and CTP in patients with acute on chronic liver failure admitted to the ward[J]. Rev Esp Enferm Dig, 2017, 109( 6): 399- 405. DOI: 10.17235/reed.2017.4701/2016. [15] ABDALLAH MA, KUO YF, ASRANI S, et al. Validating a novel score based on interaction between ACLF grade and MELD score to predict waitlist mortality[J]. J Hepatol, 2021, 74( 6): 1355- 1361. DOI: 10.1016/j.jhep.2020.12.003. [16] LI N, HUANG C, YU KK, et al. Validation of prognostic scores to predict short-term mortality in patients with HBV-related acute-on-chronic liver failure: The CLIF-C OF is superior to MELD, CLIF SOFA, and CLIF-C ACLF[J]. Medicine, 2017, 96( 17): e6802. DOI: 10.1097/MD.0000000000006802. -

 本文二维码
本文二维码
计量
- 文章访问数: 245
- HTML全文浏览量: 103
- PDF下载量: 51
- 被引次数: 0

