
 PDF下载 ( 1187 KB)
PDF下载 ( 1187 KB)

免疫球蛋白G与免疫球蛋白M比值对经导管动脉栓塞化疗联合酪氨酸激酶抑制剂和程序性细胞死亡蛋白-1抑制剂治疗的初始不可切除肝细胞癌患者预后的预测价值
DOI: 10.12449/JCH260114
Value of immunoglobulin G/immunoglobulin M ratio in predicting the prognosis of patients with initially unresectable hepatocellular carcinoma treated by transcatheter arterial chemoembolization combined with tyrosine kinase inhibitor and programmed cell death protein-1 inhibitor
-
摘要:
目的 探讨初始不可切除的肝细胞癌(iuHCC)患者接受经导管动脉栓塞化疗联合酪氨酸激酶抑制剂和程序性细胞死亡蛋白-1抑制剂三联治疗(TTP)时,免疫球蛋白G与免疫球蛋白M比值(IgG/IgM)与患者预后的关系。 方法 回顾性收集并分析2019年11月—2022年12月于广西医科大学附属肿瘤医院肝胆外科连续接受TTP三联治疗的151例iuHCC患者的临床资料。根据IgG/IgM的水平将患者分为高(IgG/IgM>13.23)、低(IgG/IgM≤13.23)两组。计量资料两组间比较采用成组t检验,计数资料两组间比较采用χ2检验。使用Kaplan-Meier法和Log-rank检验进行生存分析,采用Cox比例风险模型分析总生存期(OS)的潜在影响因素。 结果 151例患者的中位OS为26.7个月[95%置信区间(CI):19.8~未达到],中位无进展生存期(PFS)为12.5个月(95%CI:10.4~15.8)。客观缓解率为83.4%,疾病控制率为94.0%。高IgG/IgM组与低IgG/IgM组患者的基线资料差异均无统计学意义(P值均>0.05)。高IgG/IgM组患者的中位OS为20.6个月,而低IgG/IgM组患者的中位OS为未达到,差异有统计学意义(P=0.016)。高IgG/IgM组与低IgG/IgM组中,挽救性肝切除均与OS改善显著相关(χ2值分别为8.297、10.307,P值均<0.05)。多因素分析显示,高IgG/IgM[风险比(HR)=1.799,95%CI:1.077~3.006,P=0.025]、基线AFP>400 ng/mL(HR=1.762,95%CI:1.017~3.050,P=0.043)和巴塞罗那肝癌分期(HR=2.265,95%CI:1.212~4.232,P=0.010)是患者OS的独立影响因素。 结论 在接受TTP三联治疗的iuHCC患者中,高IgG/IgM与更差的预后相关,而挽救性肝切除对高IgG/IgM患者的预后改善具有潜在价值。 Abstract:Objective To investigate the association between immunoglobulin G (IgG)/immunoglobulin M (IgM) ratio and prognosis in patients with initially unresectable hepatocellular carcinoma (iuHCC) receiving TTP triple therapy with transcatheter arterial chemoembolization (TACE), tyrosine kinase inhibitor (TKI), and programmed cell death protein-1 (PD-1) inhibitors. Methods A retrospective analysis was performed for the clinical data of 151 iuHCC patients who received TTP triple therapy in Department of Hepatobiliary Surgery, Guangxi Medical University Cancer Hospital, from November 2019 to December 2022, and according to IgG/IgM ratio, they were divided into high IgG/IgM group (IgG/IgM ratio >13.23) and low IgG/IgM group (IgG/IgM ratio ≤13.23). The t-test was used for comparison of continuous data between groups, and the chi-square test was used for comparison of categorical data between groups. The Kaplan-Meier method and the log-rank test were used for survival analysis, and the Cox proportional hazards model was used to investigate the potential influencing factors for overall survival (OS). Results The 151 patients had a median OS of 26.7 months (95% confidence interval [CI]: 19.8-not reached) and a median progression-free survival of 12.5 months (95%CI: 10.4 — 15.8). The objective response rate was 83.4% and the disease control rate was 94.0%. There were no significant differences in baseline data between the high IgG/IgM group and the low IgG/IgM group (all P>0.05). There was a significant difference in median OS between the high IgG/IgM group and the low IgG/IgM group (20.6 months vs not reached, P=0.016). In both the high IgG/IgM group and the low IgG/IgM group, salvage hepatectomy was significantly associated with the improvement in OS (χ2=8.297 and 10.307, both P<0.05). The multivariate analysis showed that high IgG/IgM ratio (hazard ratio [HR]=1.799, 95%CI: 1.077 — 3.006, P=0.025), baseline alpha-fetoprotein >400 ng/mL (HR=1.762, 95%CI: 1.017 — 3.050, P=0.043), and BCLC stage (HR=2.265, 95%CI: 1.212 — 4.232, P=0.010) were independent influencing factors for OS. Conclusion High IgG/IgM ratio is associated with a poorer prognosis in iuHCC patients receiving TTP triple therapy, and salvage hepatectomy has a potential value in improving the prognosis of patients with a high IgG/IGM ratio. -
Key words:
- Carcinoma, Hepatocellular /
- Immunoglobulin G /
- Immunoglobulin M /
- Hepatectomy /
- Prognosis
-
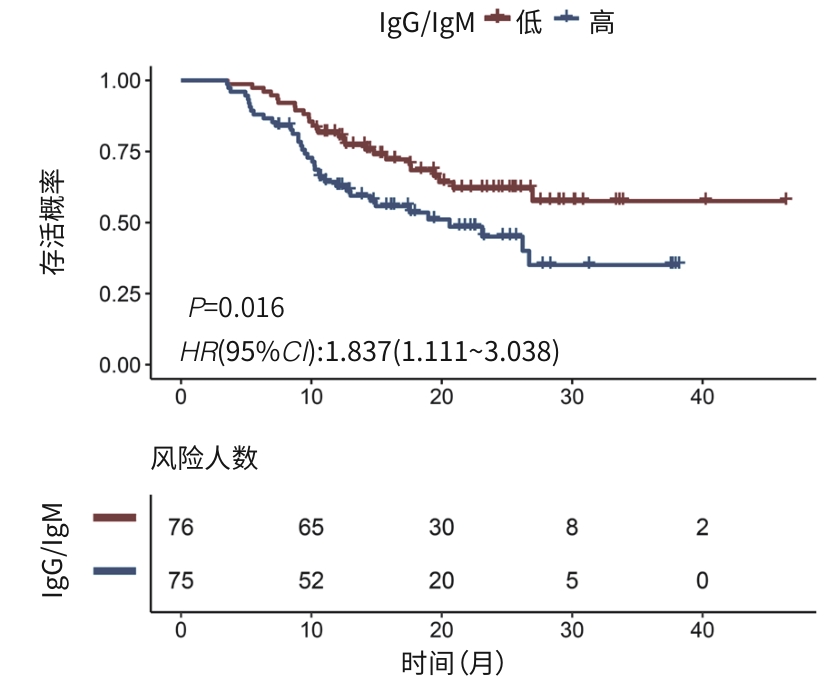
注: IgG,免疫球蛋白G;IgM,免疫球蛋白M;HR,风险比;CI,置信区间。
图 1 接受TTP三联治疗的不同IgG/IgM患者的生存曲线
Figure 1. Survival curves for patients with different IgG/IgM who received TTP triple therapy
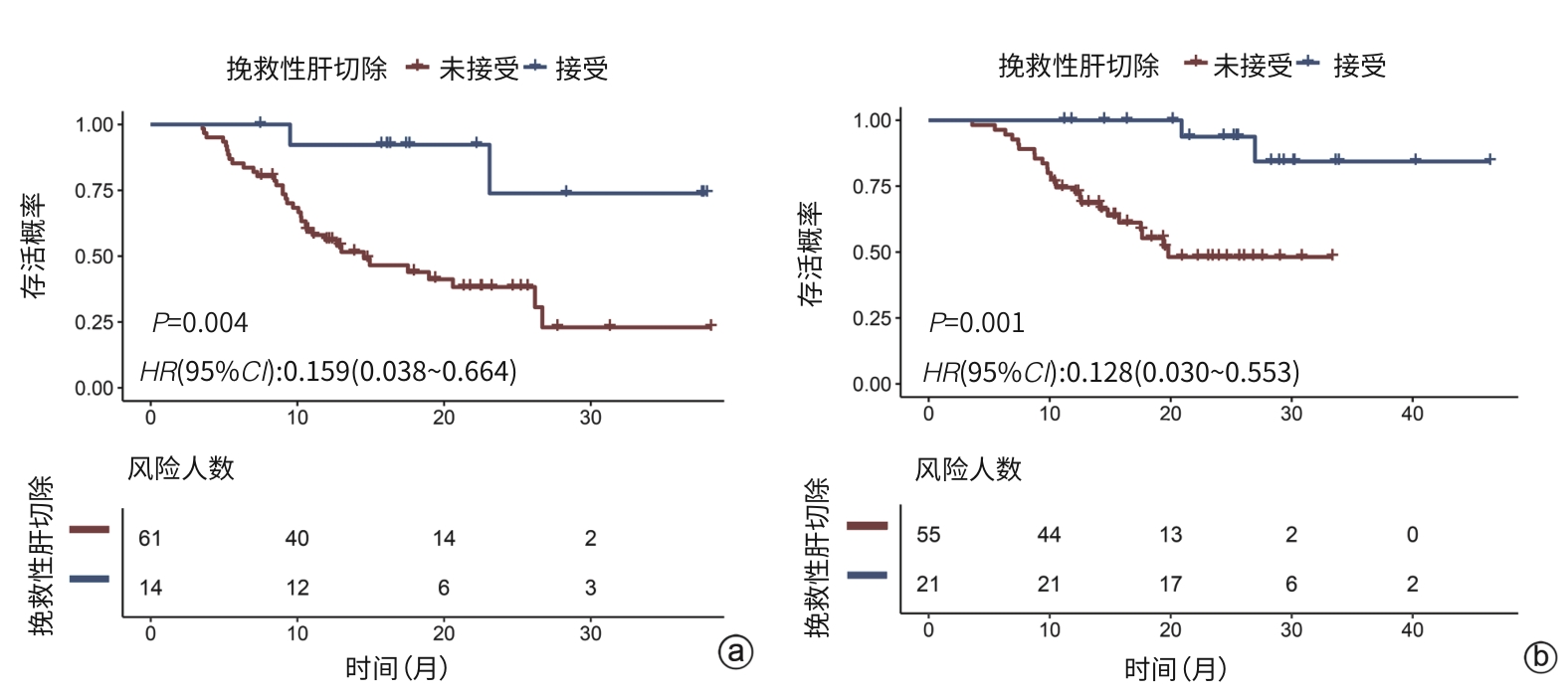
注: a,高IgG/IgM组;b,低IgG/IgM组。IgG,免疫球蛋白G;IgM,免疫球蛋白M;HR,风险比;CI,置信区间。
图 2 在高IgG/IgM组及低IgG/IgM组中根据是否接受挽救性肝切除分组的OS生存曲线
Figure 2. Survival curves of OS in the high-IgG/IgM group and the low-IgG/IgM group based on salvage hepatectomy status
表 1 接受TTP三联治疗的不可切除HCC患者的基线资料
Table 1. Baseline data for unresectable HCC patients treated with TTP triple therapy
变量 总计(n=151) 高IgG/IgM组(n=75) 低IgG/IgM组(n=76) 统计值 P值 年龄[例(%)] χ2=1.210 0.271 >60岁 27(17.9) 16(21.3) 11(14.5) ≤60岁 124(82.1) 59(78.7) 65(85.5) 性别[例(%)] χ2=2.181 0.140 男 133(88.1) 69(92.0) 64(84.2) 女 18(11.9) 6(8.0) 12(15.8) BCLC分期[例(%)] χ2=0.086 0.769 A/B期 48(31.8) 23(30.7) 25(32.9) C期 103(68.2) 52(69.3) 51(67.1) 肿瘤直径[例(%)] χ2=1.576 0.209 >10 cm 89(58.9) 48(64.0) 41(53.9) ≤10 cm 62(41.1) 27(36.0) 35(46.1) 肿瘤数目[例(%)] χ2=3.723 0.054 1个 60(39.7) 24(32.0) 36(47.4) ≥2个 91(60.3) 51(68.0) 40(52.6) 大血管侵犯 [例(%)]χ2=0.053 0.818 是 98(64.9) 48(64.0) 50(65.8) 否 53(35.1) 27(36.0) 26(34.2) 肝外转移 [例(%)]χ2=0.001 0.973 是 22(14.6) 11(14.7) 11(14.5) 否 129(85.4) 64(85.3) 65(85.5) AFP[例(%)] χ2=0.159 0.690 >400 ng/mL 89(58.9) 43(57.3) 46(60.5) ≤400 ng/mL 62(41.1) 32(42.7) 30(39.5) 乙型肝炎[例(%)] χ2=1.179 0.278 是 135(89.4) 65(86.7) 70(92.1) 否 16(10.6) 10(13.3) 6(7.9) ECOG PS[例(%)] χ2=0.833 0.361 0分 85(56.3) 45(60.0) 40(52.6) 1分 66(43.7) 30(40.0) 36(47.4) 肝硬化[例(%)] χ2=0.055 0.815 是 112(74.2) 55(73.3) 57(75.0) 否 39(25.8) 20(26.7) 19(25.0) Child-Pugh分级[例(%)] χ2=2.461 0.117 A级 126(83.4) 59(78.7) 67(88.2) B级 25(16.6) 16(21.3) 9(11.8) 凝血酶原时间(s) 12.7±1.7 12.6±1.6 12.8±1.7 t=-0.617 0.538 注:HCC,肝细胞癌;BCLC分期,巴塞罗那临床肝癌分期;AFP,甲胎蛋白;ECOG PS,东部肿瘤协作组功能状态评分;Child-Pugh分级,蔡尔德-皮尤分级;IgG,免疫球蛋白G;IgM,免疫球蛋白M。
 下载: 导出CSV
下载: 导出CSV
表 2 接受TTP三联治疗的不可切除HCC患者中OS的单因素分析
Table 2. Univariate analysis of influencing factors for OS in unresectable HCC patients treated with TTP triple therapy
变量 HR(95%CI) P值 年龄(>60岁vs ≤60岁) 0.998(0.520~1.914) 0.996 性别(男vs女) 1.316(0.599~2.892) 0.494 HBsAg阳性(是vs否) 0.872(0.397~1.916) 0.733 靶肿瘤直径(>10 cm vs ≤10 cm) 1.625(0.956~2.765) 0.073 肿瘤数目(多发vs单发) 1.656(0.974~2.816) 0.063 门静脉癌栓(是vs否) 1.678(0.998~2.820) 0.051 大血管侵犯(是vs否) 1.972(1.116~3.484) 0.019 肝外转移(是vs否) 2.235(1.229~4.066) 0.008 BCLC分期(C期vsA/B期) 2.355(1.276~4.345) 0.006 AFP(>400 ng/mL vs ≤400 ng/mL) 1.805(1.053~3.094) 0.032 PLR(>131.9 vs ≤131.9) 1.495(0.907~2.465) 0.115 HBV DNA(≥20 IU/mL vs <20 IU/mL) 0.901(0.497~1.632) 0.731 肝硬化(是vs否) 1.834(0.957~3.514) 0.068 丙氨酸氨基转移酶(>40 U/L vs ≤40 U/L) 1.065(0.647~1.753) 0.804 天冬氨酸氨基转移酶(>40 U/L vs ≤40 U/L) 1.343(0.662~2.722) 0.414 白蛋白-胆红素分级(1级 vs 2/3级) 0.870(0.349~2.169) 0.765 ECOG PS(0分 vs 1分) 1.295(0.777~2.159) 0.321 Child-Pugh分级(A级vs B级) 2.388(1.338~4.260) 0.003 CD4(>40% vs ≤40%) 0.939(0.573~1.539) 0.803 CD8(>21.3% vs ≤21.3%) 1.390(0.845~2.290) 0.195 IgG(>14.97 g/L vs ≤14.97 g/L) 1.282(0.779~2.108) 0.328 IgM(>1.21 g/L vs ≤1.21 g/L) 0.950(0.578~1.559) 0.839 CD8/CD4(>0.57 vs ≤0.57) 0.855(0.521~1.402) 0.534 IgG/IgM(>13.23 vs ≤13.23) 1.837(1.111~3.038) 0.018 注:HCC,肝细胞癌;OS,总生存期;HBsAg,乙型肝炎病毒表面抗原;BCLC分期,巴塞罗那临床肝癌分期;AFP,甲胎蛋白;PLR,血小板与淋巴细胞比值;ECOG PS,东部肿瘤协作组功能状态评分;Child-Pugh分级,蔡尔德-皮尤分级;IgG,免疫球蛋白G;IgM,免疫球蛋白M;HR,风险比;CI,置信区间。
下载: 导出CSV
表 3 接受TTP三联治疗的不可切除HCC患者中OS的多因素分析
Table 3. Multivariate analysis of influencing factors for OS in unresectable HCC patients treated with TTP triple therapy
变量 HR(95%CI) P值 模型1 BCLC分期(C期 vs A/B期) 2.265(1.212~4.232) 0.010 AFP(>400 ng/mL vs ≤400 ng/mL) 1.762(1.017~3.050) 0.043 肝硬化(是 vs 否) 1.700(0.868~3.329) 0.122 Child-Pugh分级(A级 vs B级) 1.428(0.765~2.667) 0.263 IgG/IgM(>13.23 vs ≤13.23) 1.799(1.077~3.006) 0.025 模型2 靶肿瘤直径(>10 cm vs ≤10 cm) 1.372(0.792~2.378) 0.260 肿瘤数目(多发 vs 单发) 1.402(0.796~2.469) 0.242 大血管侵犯(是 vs 否) 1.959(1.089~3.521) 0.025 肝外转移(是 vs 否) 1.606(0.842~3.062) 0.150 AFP(>400 ng/mL vs ≤400 ng/mL) 1.564(0.895~2.731) 0.116 肝硬化(是 vs 否) 1.783(0.895~3.553) 0.100 Child-Pugh分级(A级 vs B级) 1.346(0.719~2.522) 0.353 IgG/IgM(>13.23 vs ≤13.23) 1.705(1.017~2.856) 0.043 注:HCC,肝细胞癌;OS,总生存期;BCLC,巴塞罗那临床肝癌分期;AFP,甲胎蛋白;Child-Pugh分级,蔡尔德-皮尤分级;IgG,免疫球蛋白G;IgM,免疫球蛋白M;HR,风险比;CI,置信区间。模型1未纳入靶肿瘤直径、肿瘤数目、大血管侵犯和肝外转移;模型2未纳入BCLC分期。
下载: 导出CSV
-
[1] VILLANUEVA A. Hepatocellular carcinoma[J]. N Engl J Med, 2019, 380( 15): 1450- 1462. DOI: 10.1056/nejmra1713263. [2] BRAY F, FERLAY J, SOERJOMATARAM I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68( 6): 394- 424. DOI: 10.3322/caac.21492. [3] YIN L, LI H, LI AJ, et al. Partial hepatectomy vs. transcatheter arterial chemoembolization for resectable multiple hepatocellular carcinoma beyond Milan Criteria: A RCT[J]. J Hepatol, 2014, 61( 1): 82- 88. DOI: 10.1016/j.jhep.2014.03.012. [4] ARITA J, ICHIDA A, NAGATA R, et al. Conversion surgery after preoperative therapy for advanced hepatocellular carcinoma in the era of molecular targeted therapy and immune checkpoint inhibitors[J]. J Hepatobiliary Pancreat Sci, 2022, 29( 7): 732- 740. DOI: 10.1002/jhbp.1135. [5] YANG F, XU GL, HUANG JT, et al. Transarterial chemoembolization combined with immune checkpoint inhibitors and tyrosine kinase inhibitors for unresectable hepatocellular carcinoma: Efficacy and systemic immune response[J]. Front Immunol, 2022, 13: 847601. DOI: 10.3389/fimmu.2022.847601. [6] KE Q, XIN F, FANG H, et al. The significance of transarterial chemoembolization) combined with tyrosine kinase inhibitors and immune checkpoint inhibitors for unresectable hepatocellular carcinoma in the era of systemic therapy: A systematic review[J]. Front Immunol, 2022, 13( 913464. DOI: 10.3389/fimmu.2022.913464. [7] QU SP, ZHANG XB, WU YT, et al. Efficacy and safety of TACE combined with lenvatinib plus PD-1 inhibitors compared with TACE alone for unresectable hepatocellular carcinoma patients: A prospective cohort study[J]. Front Oncol, 2022, 12: 874473. DOI: 10.3389/fonc.2022.874473. [8] YANG Y, LU P, LIN KY, et al. Multi-center study on influencing factors of early recurrence of patients undergoing hepatectomy after initial unresectable hepatocellular carcinoma decline and prediction model construction[J]. Chin J Dig Surg, 2025, 24( 2): 223- 235. DOI: 10.3760/cma.j.cn115610-20250106-00011.杨云, 卢鹏, 林孔英, 等. 初始不可切除肝细胞癌降期后行肝切除术患者早期复发影响因素分析及预测模型构建的多中心研究[J]. 中华消化外科杂志, 2025, 24( 2): 223- 235. DOI: 10.3760/cma.j.cn115610-20250106-00011. [9] QU WF, DING ZB, QU XD, et al. Conversion therapy for initially unresectable hepatocellular carcinoma using a combination of toripalimab, lenvatinib plus TACE: Real-world study[J]. BJS Open, 2022, 6( 5): zrac114. DOI: 10.1093/bjsopen/zrac114. [10] YANG DL, YE L, ZENG FJ, et al. Multicenter, retrospective GUIDANCE001 study comparing transarterial chemoembolization with or without tyrosine kinase and immune checkpoint inhibitors as conversion therapy to treat unresectable hepatocellular carcinoma: Survival benefit in intermediate or advanced, but not early, stages[J]. Hepatology, 2025, 82( 2): 357- 369. DOI: 10.1097/HEP.0000000000001229. [11] LIN KY, LIN ZW, CHEN QJ, et al. Perioperative safety, oncologic outcome, and risk factors of salvage liver resection for initially unresectable hepatocellular carcinoma converted by transarterial chemoembolization plus tyrosine kinase inhibitor and anti-PD-1 antibody: A retrospective multicenter study of 83 patients[J]. Hepatol Int, 2023, 17( 6): 1477- 1489. DOI: 10.1007/s12072-023-10561-6. [12] WU JY, ZHANG ZB, ZHOU JY, et al. Outcomes of salvage surgery for initially unresectable hepatocellular carcinoma converted by transcatheter arterial chemoembolization combined with lenvatinib plus anti-PD-1 antibodies: A multicenter retrospective study[J]. Liver Cancer, 2023, 12( 3): 229- 237. DOI: 10.1159/000528356. [13] LI XZ, CHEN J, WANG XB, et al. Outcomes and prognostic factors in initially unresectable hepatocellular carcinoma treated using conversion therapy with lenvatinib and TACE plus PD-1 inhibitors[J]. Front Oncol, 2023, 13: 1110689. DOI: 10.3389/fonc.2023.1110689. [14] LI XW, FU ZG, CHEN XX, et al. Efficacy and safety of lenvatinib combined with PD-1 inhibitors plus TACE for unresectable hepatocellular carcinoma patients in China real-world[J]. Front Oncol, 2022, 12: 950266. DOI: 10.3389/fonc.2022.950266. [15] TADA T, KUMADA T, HIRAOKA A, et al. Neutrophil-lymphocyte ratio predicts early outcomes in patients with unresectable hepatocellular carcinoma treated with atezolizumab plus bevacizumab: A multicenter analysis[J]. Eur J Gastroenterol Hepatol, 2022, 34( 6): 698- 706. DOI: 10.1097/MEG.0000000000002356. [16] HONG YM, YOON KT, CHO M. Systemic immune-inflammation index predicts prognosis of sequential therapy with sorafenib and regorafenib in hepatocellular carcinoma[J]. BMC Cancer, 2021, 21( 1): 569. DOI: 10.1186/s12885-021-08124-9. [17] YANG Y, OUYANG JZ, ZHOU YZ, et al. The CRAFITY score: A promising prognostic predictor for patients with hepatocellular carcinoma treated with tyrosine kinase inhibitor and immunotherapy combinations[J]. J Hepatol, 2022, 77( 2): 574- 576. DOI: 10.1016/j.jhep.2022.03.018. [18] SCHEINER B, POMEJ K, KIRSTEIN MM, et al. Prognosis of patients with hepatocellular carcinoma treated with immunotherapy-development and validation of the CRAFITY score[J]. J Hepatol, 2022, 76( 2): 353- 363. DOI: 10.1016/j.jhep.2021.09.035. [19] MAI RY, LU TL, LU RJ, et al. C-reactive protein-albumin ratio(CAR): A more promising inflammation-based prognostic marker for patients undergoing curative hepatectomy for hepatocellular carcinoma[J]. J Inflamm Res, 2024, 17: 919- 931. DOI: 10.2147/JIR.S441623. [20] BALCAR L, BAUER D, POMEJ K, et al. Early changes in immunoglobulin G levels during immune checkpoint inhibitor treatment are associated with survival in hepatocellular carcinoma patients[J]. PLoS One, 2023, 18( 4): e0282680. DOI: 10.1371/journal.pone.0282680. [21] YI CH, WENG HL, ZHOU FG, et al. Elevated core-fucosylated IgG is a new marker for hepatitis B virus-related hepatocellular carcinoma[J]. Oncoimmunology, 2015, 4( 12): e1011503. DOI: 10.1080/2162402X.2015.1011503. [22] NAKAYA S, OGAWA R, HAYAKAWA S, et al. Serum IgG level is a predicting factor for the response to neoadjuvant chemotherapy in patients with esophageal squamous cell carcinoma[J]. World J Surg Oncol, 2021, 19( 1): 217. DOI: 10.1186/s12957-021-02290-7. [23] GUARINO M, DI COSTANZO GG, GALLOTTA A, et al. Circulating SCCA-IgM complex is a useful biomarker to predict the outcome of therapy in hepatocellular carcinoma patients[J]. Scand J Clin Lab Invest, 2017, 77( 6): 448- 453. DOI: 10.1080/00365513.2017.1336569. [24] PEPPAS I, SOLLIE S, JOSEPHS DH, et al. Serum immunoglobulin levels and the risk of bladder cancer in the AMORIS Cohort[J]. Cancer Epidemiol, 2019, 62: 101584. DOI: 10.1016/j.canep.2019.101584. [25] ZHOU J, SUN HC, WANG Z, et al. Guidelines for the diagnosis and treatment of hepatocellular carcinoma(2019 edition)[J]. Liver Cancer, 2020, 9( 6): 682- 720. DOI: 10.1159/000509424. [26] ZHOU J, SUN HC, WANG Z, et al. Guidelines for the diagnosis and treatment of primary liver cancer(2022 edition)[J]. Liver Cancer, 2023, 12( 5): 405- 444. DOI: 10.1159/000530495. [27] LI XZ, WANG XB, BAI T, et al. Conversion surgery for initially unresectable hepatocellular carcinoma using lenvatinib combined with TACE plus PD-1 inhibitor: A real-world observational study[J]. Dig Liver Dis, 2024, 56( 6): 1078- 1086. DOI: 10.1016/j.dld.2023.11.027. [28] GALLE PR, FINN RS, QIN SK, et al. Patient-reported outcomes with atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma(IMbrave150): An open-label, randomised, phase 3 trial[J]. Lancet Oncol, 2021, 22( 7): 991- 1001. DOI: 10.1016/S1470-2045(21)00151-0. [29] YAO P, CHAI JS, PAN D, et al. Clinical efficacy of improved two-step hepatectomy combined with immune targeting in the treatment of borderline resectable liver cancer[J]. Chin J Dig Surg, 2024, 23( 7): 984- 988. DOI: 10.3760/cma.j.cn115610-20240606-00278.姚鹏, 柴嘉穗, 潘登, 等. 改良二步肝切除联合免疫靶向治疗临界可切除肝癌的临床疗效[J]. 中华消化外科杂志, 2024, 23( 7): 984- 988. DOI: 10.3760/cma.j.cn115610-20240606-00278. [30] KUDO M, REN ZG, GUO YB, et al. Transarterial chemoembolisation combined with lenvatinib plus pembrolizumab versus dual placebo for unresectable, non-metastatic hepatocellular carcinoma(LEAP-012): A multicentre, randomised, double-blind, phase 3 study[J]. Lancet, 2025, 405( 10474): 203- 215. DOI: 10.1016/S0140-6736(24)02575-3. [31] IPP T, MACNAB GM, GEDDES EW, et al. Serum immunoglobulin levels in primary liver cancer: Relationship to underlying cirrhosis and hepatitis-B(surface) antigenaemia[J]. Br J Cancer, 1975, 32( 4): 509- 511. DOI: 10.1038/bjc.1975.253. [32] MONROY-IGLESIAS MJ, CRESCIOLI S, BECKMANN K, et al. Antibodies as biomarkers for cancer risk: A systematic review[J]. Clin Exp Immunol, 2022, 209( 1): 46- 63. DOI: 10.1093/cei/uxac030. [33] OLUBUYIDE IO, SALIMONU LS, ADENIRAN SO. Soluble immune complexes and immunoglobulin(IgG, IgA and IgM) levels in Nigerians with primary liver cell carcinoma[J]. Afr J Med Med Sci, 1993, 22( 4): 57- 62. [34] GÜRE AO, STOCKERT E, SCANLAN MJ, et al. Serological identification of embryonic neural proteins as highly immunogenic tumor antigens in small cell lung cancer[J]. Proc Natl Acad Sci USA, 2000, 97( 8): 4198- 4203. DOI: 10.1073/pnas.97.8.4198. [35] TAYLOR DD, GERCEL-TAYLOR C. Tumor-reactive immunoglobulins in ovarian cancer: Diagnostic and therapeutic significance?(review)[J]. Oncol Rep, 1998, 5( 6): 1519- 1524. DOI: 10.3892/or.5.6.1519. [36] CHEN ZH, ZHANG GP, REN XX, et al. Cross-talk between myeloid and B cells shapes the distinct microenvironments of primary and secondary liver cancer[J]. Cancer Res, 2023, 83( 21): 3544- 3561. DOI: 10.1158/0008-5472.CAN-23-0193. [37] QIU XY, ZHU XH, ZHANG L, et al. Human epithelial cancers secrete immunoglobulin g with unidentified specificity to promote growth and survival of tumor cells[J]. Cancer Res, 2003, 63( 19): 6488- 6495. [38] LIU CX, ZHAO HR, WANG P, et al. The combination of circulating IgM and geriatric nutritional risk index predicts the prognostic of hepatocellular carcinoma patients who underwent immune checkpoint inhibitors[J]. Int Immunopharmacol, 2023, 123: 110704. DOI: 10.1016/j.intimp.2023.110704. [39] LI X, HAN QC, YU C, et al. C-C chemokine hepatocellular carcinoma motif ligand 5-deficiency promotes hepatocellular carcinoma progression by affecting B cell recruitment[J]. J Dig Dis, 2021, 22( 7): 433- 441. DOI: 10.1111/1751-2980.12997. [40] ZHU XD, HUANG C, SHEN YH, et al. Downstaging and resection of initially unresectable hepatocellular carcinoma with tyrosine kinase inhibitor and anti-PD-1 antibody combinations[J]. Liver Cancer, 2021, 10( 4): 320- 329. DOI: 10.1159/000514313. [41] LIU JW, ZHU XD, PAN YX, et al. Prognoses of patients treated with surgical therapy versus continuation of local-plus-systemic therapy following successful down-staging of intermediate-advanced hepatocellular carcinoma: A multicenter real-world study[J]. Oncologist, 2024, 29( 4): e487- e497. DOI: 10.1093/oncolo/oyad277. -

 本文二维码
本文二维码
计量
- 文章访问数: 359
- HTML全文浏览量: 156
- PDF下载量: 173
- 被引次数: 0

