
 PDF下载 ( 1131 KB)
PDF下载 ( 1131 KB)

急性坏死性胰腺炎患者发生下肢深静脉血栓的影响因素及风险评估模型的有效性分析
DOI: 10.12449/JCH260320
Risk factors for lower extremity deep vein thrombosis in patients with acute necrotizing pancreatitis and effectiveness of risk assessment models
-
摘要:
目的 探讨急性坏死性胰腺炎(ANP)患者发生下肢深静脉血栓(DVT)的影响因素,识别其独立危险因素,比较三种常用血栓风险评估模型(Caprini评分、Padua评分与Wells评分)在ANP患者中预测DVT的有效性,以期为临床识别高危人群并优化防治策略提供参考依据。 方法 回顾性收集2013年4月—2024年4月泸州市人民医院与西南医科大学附属医院收治的320例ANP患者的临床资料,根据住院期间是否发生DVT分为血栓组(n=25)和对照组(n=295)。使用倾向性评分匹配分析比较2组患者的既往史及住院期间各项检查结果,通过单因素和多因素Logistic回归分析ANP患者住院期间下肢DVT形成的危险因素,并基于独立影响因素建立DVT风险评估模型,进一步通过受试者操作特征曲线评估模型性能。计算并采用DeLong检验比较曲线下面积(AUC)、敏感度及特异度。计量资料两组间比较采用成组t检验或Mann-Whitney U检验;计数资料组间比较采用χ2检验。 结果 倾向性评分匹配后血栓组24例,对照组112例。两组临床特征分析结果显示,血栓组患者的胰腺坏死程度、D-二聚体水平、急性胰腺炎严重程度床旁指数(BISAP)评分、透析史占比均高于对照组患者(P值均<0.05)。多因素Logistic回归分析结果显示,BISAP评分、胰腺坏死程度、D-二聚体水平是ANP患者住院期间发生下肢DVT的独立危险因素(P值均<0.05)。BISAP评分+Caprini评分预测患者下肢DVT风险的AUC为0.832(95%置信区间:0.722~0.942,P<0.001),约登指数为1.661,最佳截断值为0.26,敏感度和特异度分别为75.0%和91.1%。 结论 D-二聚体、BISAP评分、胰腺坏死程度是ANP患者住院期间发生下肢DVT的独立危险因素,BISAP评分+Caprini评分评估模型能够有效预测ANP患者的DVT风险。 -
关键词:
- 胰腺炎, 急性坏死性 /
- 静脉血栓形成 /
- 危险因素
Abstract:Objective To investigate the influencing factors and independent risk factors for lower extremity deep vein thrombosis (DVT) in patients with acute necrotizing pancreatitis (ANP), to analyze the effectiveness of three commonly used risk assessment models for thrombosis (Caprini score, Padua score, and Wells score), and to provide a reference for clinical identification of high-risk individuals and optimization of prevention and treatment strategies. Methods A retrospective analysis was performed for the clinical data of 320 patients with ANP who were admitted to Luzhou People’s Hospital and The Affiliated Hospital of Southwest Medical University from April 2013 to April 2024, and according to the presence or absence of DVT during hospitalization, the patients were divided into thrombosis group with 25 patients and control group with 295 patients. After propensity score matching, the two groups were compared in terms of past history and various examination results during hospitalization. The risk factors for lower extremity DVT in ANP patients during hospitalization were analyzed through univariate and multivariate Logistic regression, and a DVT risk prediction model was established based on independent influencing factors. The receiver operating characteristic (ROC) curve was used to assess the performance of models, and the DeLong test was used for comparison of the area under the ROC curve (AUC), sensitivity, and specificity. The independent-samples t test or the Mann-Whitney U test was used for comparison of continuous data between two groups; the chi-square test was used for comparison of categorical data between groups. Results After matching, the patients were divided into thrombosis group with 24 patients and control group with 112 patients. The clinical characteristics analysis showed that compared with the control group, the thrombosis group had significantly higher degree of pancreatic necrosis, D-dimer level, Bedside Index for Severity in Acute Pancreatitis (BISAP) score, and proportion of patients undergoing dialysis (all P<0.05). The multivariable Logistic regression analysis showed that BISAP score, degree of pancreatic necrosis, and D-dimer level were independent risk factors for lower extremity DVT in ANP patients during hospitalization (all P<0.05). The BISAP-Caprini score model had an AUC of 0.832 (95% confidence interval: 0.722 — 0.942, P<0.001) in predicting the risk of lower extremity DVT, with a Youden index of 1.661, an optimal cut-off value of 0.26, a sensitivity of 75.0%, and a specificity of 91.1%. Conclusion D-dimer, BISAP score, and the degree of pancreatic necrosis are independent risk factors for lower extremity DVT in patients with ANP during hospitalization, and the BISAP-Caprini score model can effectively predict the risk of DVT in ANP patients. -
Key words:
- Pancreatitis, Acute Necrotizing /
- Venous Thrombosis /
- Risk Factors
-
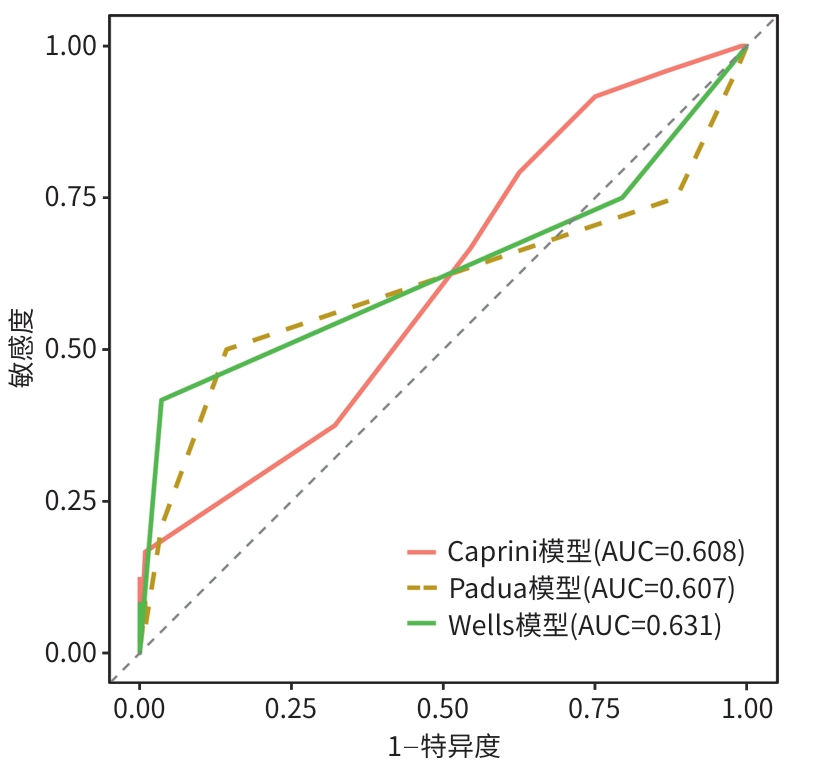
注: ROC曲线,受试者操作特征曲线。
图 1 3种血栓风险评估模型的ROC曲线
Figure 1. ROC curves of three thrombus risk assessment models
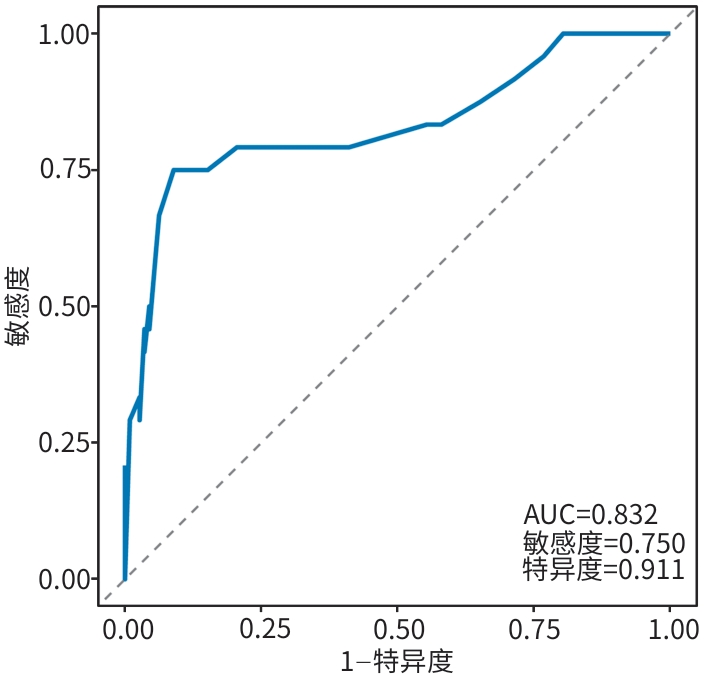
注: BISAP,急性胰腺炎严重程度床旁指数;ROC曲线,受试者操作特征曲线。
图 2 BISAP评分联合Caprini评分构建预测模型的ROC曲线
Figure 2. ROC curve of the prediction model constructed by combining BISAP score and Caprini score
表 1 ANP患者的基线临床特征
Table 1. Baseline clinical characteristics of ANP patients
变量 匹配前 匹配后 总计(n=320) 对照组(n=295) 血栓组(n=25) 统计值 P值 总计(n=136) 对照组(n=112) 血栓组(n=24) 统计值 P值 性别[例(%)] 203(64.40) 191(64.70) 12(48.00) χ2 =2.11 0.146 71(52.20) 59(52.70) 12(50.00) χ2 =0.00 0.989 年龄(岁) 48(38~58) 48(38~57) 51(40~71) W=3 038.00 0.144 52(41~62) 52(41~61) 51(40~70) W=1 260.00 0.636 吸烟史[例(%)] 118(36.90) 110(37.30) 8(32.00) χ2 =0.10 0.756 46(33.80) 38(33.90) 8(33.30) χ2 =0.00 >0.05 饮酒史[例(%)] 133(41.60) 125(42.40) 8(32.00) χ2 =0.64 0.424 47(34.60) 39(34.80) 8(33.30) χ2 =0.00 >0.05 高血压病史[例(%)] 99(30.90) 87(29.50) 12(48.00) χ2 =2.88 0.090 51(37.50) 40(35.70) 11(45.80) χ2 =0.49 0.486 糖尿病病史[例(%)] 90(28.10) 82(27.80) 8(32.00) χ2 =0.05 0.828 38(27.90) 30(26.80) 8(33.30) χ2 =0.16 0.691 BMI(kg/m2) 26.64±3.47 26.51±3.44 28.06±3.56 t=-2.16 0.032 27.94±2.81 27.93±2.62 27.99±3.61 t=-0.09 0.924 胰腺坏死程度(%) 10.00
(10.00~20.00)10.00
(10.00~10.00)30.00
(10.00~30.00)W=2 184.00 <0.001 0.10
(0.10~0.20)0.10
(0.10~0.10)0.25
(0.10~0.30)W=688.00 <0.001 血糖(mmol/L) 8.88
(6.67~13.00)8.60
(6.70~13.00)9.92
(8.17~18.00)W=2 768.00 0.038 9.00
(6.88~13.36)8.78
(6.79~13.07)9.77
(8.08~17.29)W=1 073.00 0.123 总胆固醇(mmol/L) 5.27
(3.83~8.08)5.46
(3.84~8.37)4.77
(3.76~6.16)W=4 228.00 0.212 4.76
(3.44~6.43)4.75
(3.37~6.83)4.89
(3.76~6.19)W=1 304.50 0.824 甘油三酯(mmol/L) 3.68
(1.52~15.52)3.67
(1.54~16.06)3.74
(1.48~7.88)W=3 866.00 0.667 2.83
(1.40~7.90)2.68
(1.40~8.01)3.90
(1.44~7.90)W=1 272.00 0.683 白蛋白(g/L) 39.40
(34.30~43.32)39.60
(34.65~43.50)35.40
(31.40~41.50)W=4 736.00 0.018 38.75
(33.27~42.12)39.25
(33.88~42.32)35.95
(31.35~41.55)W=1 616.00 0.120 ALT(U/L) 34.00
(20.20~66.62)34.00
(20.09~67.75)38.00
(18.30~48.50)W=3 750.00 0.890 36.20
(20.65~83.15)35.90
(21.00~89.17)38.75
(17.73~54.38)W=1 436.00 0.599 肌酐(μmol/L) 66.00
(51.00~81.40)65.00
(50.10~80.80)75.00
(58.00~104.00)W=2 667.00 0.021 66.00
(49.72~83.65)65.00
(48.00~77.52)75.50
(58.00~105.60)W=956.00 0.026 CRP(mg/L) 80.94
(23.00~178.81)78.00
(23.00~174.48)94.07
(20.10~182.54)W=3 370.00 0.776 84.97
(32.01~179.46)84.97
(33.31~165.97)88.47
(20.10~182.54)W=1 356.00 0.950 WBC(×109/L) 12.94
(9.52~16.24)12.93
(9.50~16.21)14.09
(10.59~18.53)W=3 338.00 0.443 12.93
(9.29~16.75)12.79
(9.06~16.33)13.82
(10.40~18.67)W=1 264.00 0.689 D-二聚体(mg/L) 2.58
(1.40~5.60)2.40
(1.30~4.94)9.80
(7.16~14.34)W=1 006.00 <0.001 3.46
(1.52~7.44)2.83
(1.49~5.25)9.57
(7.14~14.86)W=427.00 <0.001 BISAP评分(分) 1.00
(1.00~1.00)1.00
(0.00~1.00)2.00
(2.00~3.00)W=1 054.00 <0.001 1.00
(1.00~1.25)1.00
(1.00~1.00)2.00
(1.75~3.00)W=454.00 <0.001 透析史[例(%)] 21(6.60) 16(5.40) 5(20.00) χ2 =5.79 0.016 10(7.40) 5(4.50) 5(20.80) χ2 =5.56 0.018 注:ANP,急性坏死性胰腺炎;BMI,体重指数;ALT,丙氨酸氨基转移酶;CRP,C反应蛋白;WBC,白细胞计数;BISAP,急性胰腺炎严重程度床旁指数。
 下载: 导出CSV
下载: 导出CSV
表 2 ANP患者发生下肢DVT影响因素的Logistic回归分析
Table 2. Multivariate Logistic regression analysis of influencing factors of lower extremity DVT in patients with ANP
变量 单因素分析 多因素分析 OR 95%CI P值 OR 95%CI P值 性别 1.113 0.457~2.712 0.812 年龄 1.011 0.982~1.040 0.455 1.000 0.959~1.042 0.993 吸烟史 0.974 0.366~2.426 0.955 饮酒史 0.936 0.352~2.329 0.889 高血压病史 1.523 0.616~3.721 0.355 糖尿病病史 1.367 0.509~3.451 0.518 BMI 1.008 0.862~1.185 0.923 胰腺坏死程度 1.027 0.994~1.061 0.107 1.056 1.010~1.111 0.022 血糖 1.047 0.986~1.109 0.122 总胆固醇 1.002 0.903~1.076 0.968 甘油三酯 0.993 0.955~1.020 0.663 白蛋白 0.933 0.865~1.002 0.063 ALT 0.998 0.992~1.002 0.402 肌酐 1.003 1.000~1.007 0.061 CRP 1.000 0.995~1.004 0.985 WBC 1.024 0.954~1.096 0.492 D-二聚体 1.259 1.151~1.398 <0.001 1.217 1.087~1.390 0.001 BISAP评分 4.866 2.718~9.841 <0.001 3.730 1.868~8.544 <0.001 透析史 5.632 1.442~22.128 0.011 2.544 0.256~22.511 0.409 注:因发生ANP的病因有高脂血症、胆道结石等,且ANP为消耗性疾病,此类患者血糖波动大、炎症重、腹腔内脏器水肿导致体循环减少、腹压升高,引起肾功能不全,故观察指标中纳入血糖、总胆固醇、甘油三酯、白蛋白、ALT、肌酐、CRP、WBC。ANP,急性坏死性胰腺炎;DVT,深静脉血栓形成;BMI,体重指数;ALT,丙氨酸氨基转移酶;CRP,C反应蛋白;WBC,白细胞计数;BISAP,急性胰腺炎严重程度床旁指数;OR,比值比;95%CI,95%置信区间。
下载: 导出CSV
表 3 BISAP+Caprini双评分模型的风险分层与DVT风险的关系
Table 3. Relationship between risk stratification in BISAP+Caprini model and risk of VTE
风险分层 对照组
(n=112)血栓组
(n=24)OR(95%CI) P值 低危组 102 6 1.00 高危组 10 18 30.60 (10.46~102.45) <0.001
下载: 导出CSV
-
[1] GLIEM N, AMMER-HERRMENAU C, ELLENRIEDER V, et al. Management of severe acute pancreatitis: An update[J]. Digestion, 2021, 102( 4): 503- 507. DOI: 10.1159/000506830. [2] WU HS, MA KQ, LIAO BL, et al. Guiding effect of noninvasive monitoring of cardiac output and central venous oxygen saturation on early goal-directed fluid resuscitation in hyperlipidemic severe acute pancreatitis[J]. J Clin Hepatol, 2022, 38( 7): 1602- 1607. DOI: 10.3969/j.issn.1001-5256.2022.07.026.巫泓生, 马克强, 廖碧玲, 等. 无创心排量联合中心静脉血氧饱和度监测对高脂血症性重症胰腺炎早期目标导向性液体复苏的指导作用[J]. 临床肝胆病杂志, 2022, 38( 7): 1602- 1607. DOI: 10.3969/j.issn.1001-5256.2022.07.026. [3] ZHAO CS, YAO WJ, YUAN P, et al. Time distribution of risk factors for secondary pancreatic infection in acute pancreatitis[J]. J Clin Hepatol, 2022, 38( 7): 1686- 1690. DOI: 10.3969/j.issn.1001-5256.2022.07.044.赵成思, 姚维杰, 袁鹏, 等. 急性胰腺炎继发胰腺感染的危险因素及其时间分布[J]. 临床肝胆病杂志, 2022, 38( 7): 1686- 1690. DOI: 10.3969/j.issn.1001-5256.2022.07.044. [4] SURYAWANSHI G, JONASON DE, MUNIGALA S, et al. Incidence and risk factors for deep vein thrombosis(DVT) and pulmonary embolism(PE) in acute necrotizing pancreatitis(ANP)-A single center experience[J]. Pancreatology, 2024, 24( 6): 856- 862. DOI: 10.1016/j.pan.2024.07.007. [5] CHUNG WS, LIN CL. Association between venous thromboembolism and acute pancreatitis: An analysis from the nationwide inpatient sample[J]. Clin Respir J, 2020, 14( 4): 320- 327. DOI: 10.1111/crj.13134. [6] AHMAD DS, MANSOOR E, ALIKHAN MM, et al. Risk of venous thromboembolism in acute necrotizing pancreatitis: A large database study[J]. Pancreas, 2021, 50( 1): 71- 76. DOI: 10.1097/MPA.0000000000001714. [7] CHENG JH, LIU ZD. Incidence and risk factors of lower extremity deep venous thrombosis in severe acute pancreatitis patients during intensive care unit period[J]. J Clin Emerg, 2021, 22( 9): 597- 602. DOI: 10.13201/j.issn.1009-5918.2021.09.006.程家浩, 刘正东. 重症急性胰腺炎患者ICU期间下肢深静脉血栓形成的发生率和危险因素分析[J]. 临床急诊杂志, 2021, 22( 9): 597- 602. DOI: 10.13201/j.issn.1009-5918.2021.09.006. [8] BANKS PA, BOLLEN TL, DERVENIS C, et al. Classification of acute pancreatitis 2012: revision of the Atlanta classification and definitions by international consensus[J]. Gut, 2013, 62( 1): 102- 111. DOI: 10.1136/gutjnl-2012-302779. [9] LUO XP, WANG J, WU Q, et al. Research advances in acute pancreatitis scoring system[J]. J Clin Hepatol, 2022, 38( 9): 2188- 2192. DOI: 10.3969/j.issn.1001-5256.2022.09.046.罗秀平, 王洁, 吴青, 等. 急性胰腺炎评分系统的研究进展[J]. 临床肝胆病杂志, 2022, 38( 9): 2188- 2192. DOI: 10.3969/j.issn.1001-5256.2022.09.046. [10] WU BU, JOHANNES RS, SUN X, et al. The early prediction of mortality in acute pancreatitis: a large population-based study[J]. Gut, 2008, 57( 12): 1698- 1703. DOI: 10.1136/gut.2008.152702. [11] SAMANTA J, DHAR J, GUPTA P, et al. Venous thrombosis in acute pancreatitis: What to and not to do[J]. Dig Dis Sci, 2024, 69( 5): 1537- 1550. DOI: 10.1007/s10620-024-08418-5. [12] SINGH RR, THANDASSERY RB, CHAWLA S. Acute venous thromboembolism is common following acute necrotizing pancreatitis and is associated with worse clinical outcomes[J]. Pancreas, 2024, 53( 10): e802- e807. DOI: 10.1097/MPA.0000000000002375. [13] WENGER N, SEBASTIAN T, ENGELBERGER RP, et al. Pulmonary embolism and deep vein thrombosis: Similar but different[J]. Thromb Res, 2021, 206: 88- 98. DOI: 10.1016/j.thromres.2021.08.015. [14] Pulmonary Embolism& Pulmonary Vascular Diseases Group of the Chinese Thoracic Society, Pulmonary Embolism& Pulmonary Vascular Disease Working Group of Chinese Association of Chest Physicians, National Cooperation Group on Prevention& Treatment of Pulmonary Embolism& Pulmonary Vascular Disease. Chinese guidelines for the diagnosis, treatment, prophylaxis and management of pulmonary thromboembolism(2025 edition)[J]. Natl Med J China, 2025, 105( 26): 2162- 2194. DOI: 10.3760/cma.j.cn112137-20250509-01141.中华医学会呼吸病学分会肺栓塞与肺血管病学组, 中国医师协会呼吸医师分会肺栓塞与肺血管病工作委员会, 全国肺栓塞与肺血管病防治协作组. 中国肺血栓栓塞症诊治、预防和管理指南(2025版)[J]. 中华医学杂志, 2025, 105( 26): 2162- 2194. DOI: 10.3760/cma.j.cn112137-20250509-01141. [15] TRIKUDANATHAN G, UMAPATHY C, MUNIGALA S, et al. Venous thromboembolism is associated with adverse outcomes in hospitalized patients with acute pancreatitis: A population-based cohort study[J]. Pancreas, 2017, 46( 9): 1165- 1172. DOI: 10.1097/MPA.0000000000000906. [16] GLAUBITZ J, ASGARBEIK S, LANGE R, et al. Immune response mechanisms in acute and chronic pancreatitis: Strategies for therapeutic intervention[J]. Front Immunol, 2023, 14: 1279539. DOI: 10.3389/fimmu.2023.1279539. [17] KELLER K, SIVANATHAN V, FARMAKIS IT, et al. Incidence and impact of venous thromboembolism in hospitalized patients with acute pancreatitis[J]. Dig Liver Dis, 2024, 56( 12): 2085- 2094. DOI: 10.1016/j.dld.2024.06.023. [18] ROCH AM, MAATMAN TK, CARR RA, et al. Venous thromboembolism in necrotizing pancreatitis: An underappreciated risk[J]. J Gastrointest Surg, 2019, 23( 12): 2430- 2438. DOI: 10.1007/s11605-019-04124-0. [19] CAPURSO G, PONZ DE LEON PISANI R, LAURI G, et al. Clinical usefulness of scoring systems to predict severe acute pancreatitis: A systematic review and meta-analysis with pre and post-test probability assessment[J]. United European Gastroenterol J, 2023, 11( 9): 825- 836. DOI: 10.1002/ueg2.12464. [20] ALI H, MOOND V, VIKASH F, et al. Risk score to predict inpatient mortality of acute pancreatitis patients admitted to the intensive care unit[J]. Pancreatology, 2024, 24( 8): 1213- 1218. DOI: 10.1016/j.pan.2024.10.010. [21] ZHU JP, WU LF, WANG Y, et al. Predictive value of the Ranson and BISAP scoring systems for the severity and prognosis of acute pancreatitis: A systematic review and meta-analysis[J]. PLoS One, 2024, 19( 4): e0302046. DOI: 10.1371/journal.pone.0302046. [22] PANDOR A, TONKINS M, GOODACRE S, et al. Risk assessment models for venous thromboembolism in hospitalised adult patients: A systematic review[J]. BMJ Open, 2021, 11( 7): e045672. DOI: 10.1136/bmjopen-2020-045672. [23] ROCHA D, LOBATO CT, MELO PINTO D, et al. Venous thromboembolism prophylaxis in medical and surgical patients- what’s our reality[J]. Cureus, 2023, 15( 11): e49444. DOI: 10.7759/cureus.49444. [24] CHEN XL, HUANG JL, LIU JX, et al. Venous thromboembolism risk factors and prophylaxis of elderly intensive care unit patients in a Chinese general hospital[J]. Ann Palliat Med, 2021, 10( 4): 4453- 4462. DOI: 10.21037/apm-21-464. [25] ZHANG X, HAO AQ, LU YH, et al. Deep vein thrombosis and validation of the Caprini risk assessment model in Chinese orthopaedic trauma patients: A multi-center retrospective cohort study enrolling 34, 893 patients[J]. Eur J Trauma Emerg Surg, 2023, 49( 4): 1863- 1871. DOI: 10.1007/s00068-023-02265-1. [26] ZHOU H, HU Y, LI X, et al. Assessment of the risk of venous thromboembolism in medical inpatients using the padua prediction score and caprini risk assessment model[J]. J Atheroscler Thromb, 2018, 25( 11): 1091- 1104. DOI: 10.5551/jat.43653. [27] XIONG W, CHENG Y, ZHAO YF. Risk scores in venous thromboembolism guidelines of ESC, ACCP, and ASH: An updated review[J]. Clin Appl Thromb Hemost, 2024, 30: 10760296241263856. DOI: 10.1177/10760296241263856. [28] SUN JM, SONG JM, PAN JH, et al. Analysis of treatment strategies and safety for acute deep vein thrombosis of the lower extremities[J]. Chin J Med Offic, 2025, 53( 10): 1019- 1023, 1028. DOI: 10.16680/j.1671-3826.2025.10.06.孙健铭, 宋家明, 潘江皓, 等. 急性下肢深静脉血栓形成治疗策略及安全性分析[J]. 临床军医杂志, 2025, 53( 10): 1019- 1023, 1028. DOI: 10.16680/j.1671-3826.2025.10.06. -

 本文二维码
本文二维码
计量
- 文章访问数: 269
- HTML全文浏览量: 69
- PDF下载量: 121
- 被引次数: 0

