
 PDF下载 ( 10884 KB)
PDF下载 ( 10884 KB)

外科辅助经颈静脉肝内门体分流术治疗门静脉高压合并复杂门静脉血栓的效果及安全性分析
DOI: 10.12449/JCH260313
Efficacy and safety of surgery-assisted transjugular intrahepatic portosystemic shunt in treatment of portal hypertension comorbid with complex portal vein thrombosis
-
摘要:
目的 探讨外科辅助经颈静脉肝内门体分流术(SA-TIPS)在门静脉高压合并复杂门静脉血栓(包括门静脉海绵样变)治疗中的可行性、安全性及疗效。 方法 选取2023年11月—2025年1月首都医科大学附属北京世纪坛医院收治的36例行SA-TIPS治疗的门静脉高压合并复杂门静脉血栓患者,统计并分析患者的一般情况、手术过程的技术资料(手术成功率、穿刺针数、手术时间、支架使用数量和分流道长度)、围手术期并发症及手术恢复情况等。比较分流术前后门静脉压力梯度(PPG)变化,计算PPG下降达标率和术后1周内支架通畅率。计量资料两组间比较采用配对样本t检验。 结果 36例患者中,34例(94.4%)成功实施SA-TIPS。围手术期并发症发生率为16.7%(6/36),包括胸腹腔出血3例,术中心律失常2例,切口感染1例。SA-TIPS分流后PPG较术前显著下降(t=19.85,P<0.01),其中PPG下降幅度≥50%的患者占76.5%(26/34),1周内影像学复查分流道通畅率为100%。 结论 SA-TIPS治疗合并复杂门静脉血栓(包括门静脉海绵样变)的门静脉高压具有技术成功率高、安全有效的优势,值得临床推广。 -
关键词:
- 高血压, 门静脉 /
- 门静脉血栓 /
- 门体分流术, 经颈静脉肝内 /
- 外科手术
Abstract:Objective To investigate the feasibility, safety, and efficacy of surgery-assisted transjugular intrahepatic portosystemic shunt (SA-TIPS) in the treatment of portal hypertension comorbid with complex portal vein thrombosis, including cavernous transformation of the portal vein (CTPV). Methods An analysis was performed for the data of 36 patients with portal hypertension and complex portal vein thrombosis who underwent SA-TIPS in Beijing Shijitan Hospital, Capital Medical University, from November 2023 to January 2025, including general status, technical data of the surgical process (surgical success rate, puncture times, time of operation, the number of stents used, and the length of shunt), perioperative complications, and surgical recovery. The change in portal pressure gradient (PPG) after shunt was compared, and the rate of reaching the standard for PPG reduction was calculated, as well as stent patency rate within 1 week after surgery. The paired samples t-test was used for comparison of continuous data between two groups. Results Among the 36 patients, 34 (94.4%) underwent SA-TIPS successfully. The incidence rate of perioperative complications was 16.7% (6/36), including 3 cases of thoraco-abdominal hemorrhage, 2 cases of intraoperative arrhythmia, and 1 case of incision infection. There was a significant reduction in PPG after SA-TIPS (t=19.85, P<0.01), and the patients achieving a ≥50% reduction in PPG accounted for 76.5% (26/34). Imaging reexamination within 1 week showed a shunt patency rate of 100%. Conclusion SA-TIPS has a high technical success rate, a favorable safety profile, and good efficacy in the treatment of portal hypertension comorbid with complex portal vein thrombosis (including CTPV), and therefore, it holds promise for clinical application. -
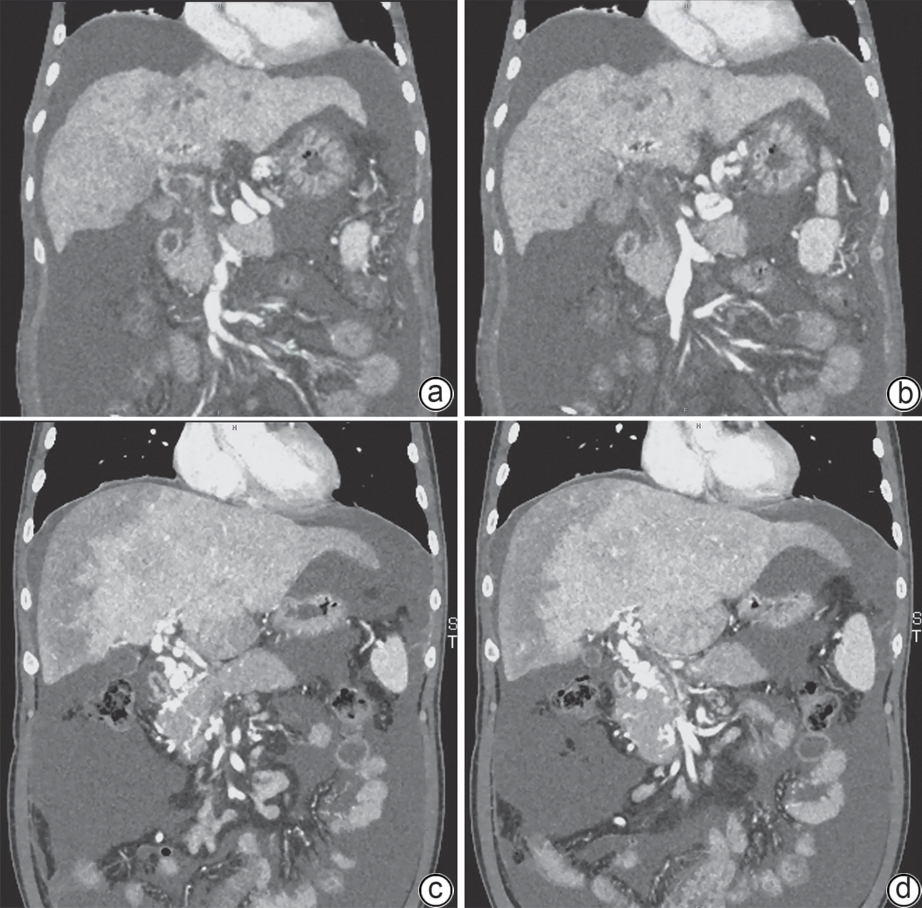
注: a、b,病例1,患者男性,36岁,乙型肝炎肝硬化,门静脉完全闭塞伴侧支形成,肝内门静脉分支显示不清;c、d,病例2,患者男性,43岁,阵发性睡眠性血红蛋白尿,门静脉血栓形成,门静脉海绵样变,大量侧支形成,固有门静脉主干及其分支纤细且被血栓填充闭塞。CT,计算机体层成像。
图 1 复杂门静脉血栓患者冠状位CT
Figure 1. Coronal CT image of patients with complex portal vein thrombosis
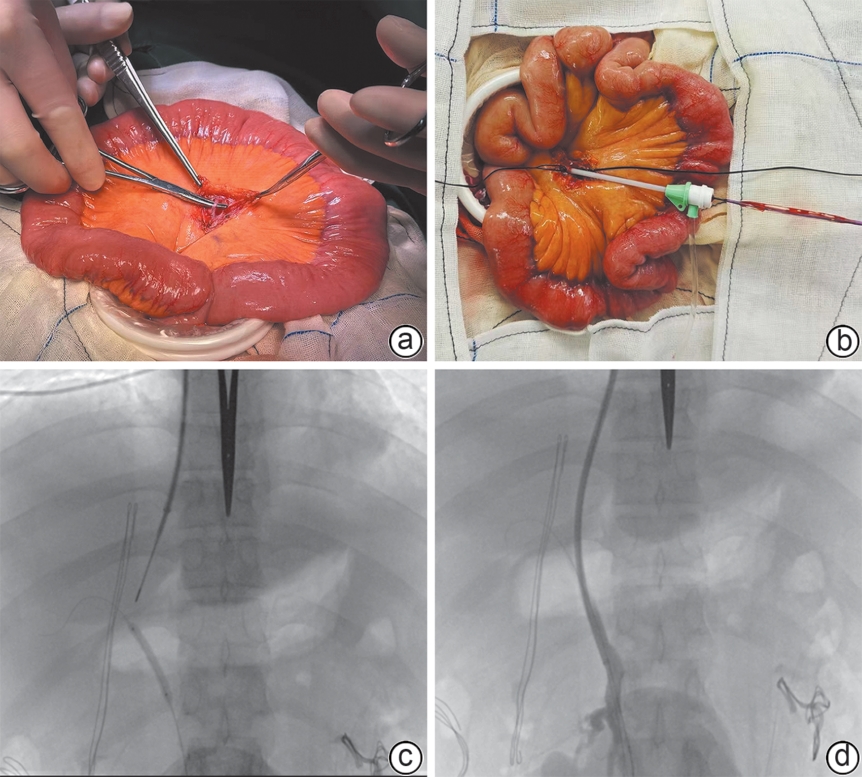
注: a,病例2,小切口进入腹腔,寻找小肠目标段,分离暴露肠系膜上静脉属支;b、c,插管进入肠系膜静脉后,在导丝进入目标血管后,置入定位球囊,颈静脉插管置入导管和穿刺针;d,鞘芯和球囊配合引导支架鞘管进入门静脉,后续再置入TIPS支架。SA-TIPS,外科辅助经颈静脉肝内门体分流术。
图 2 SA-TIPS手术部分过程
Figure 2. Partial process of SA-TIPS
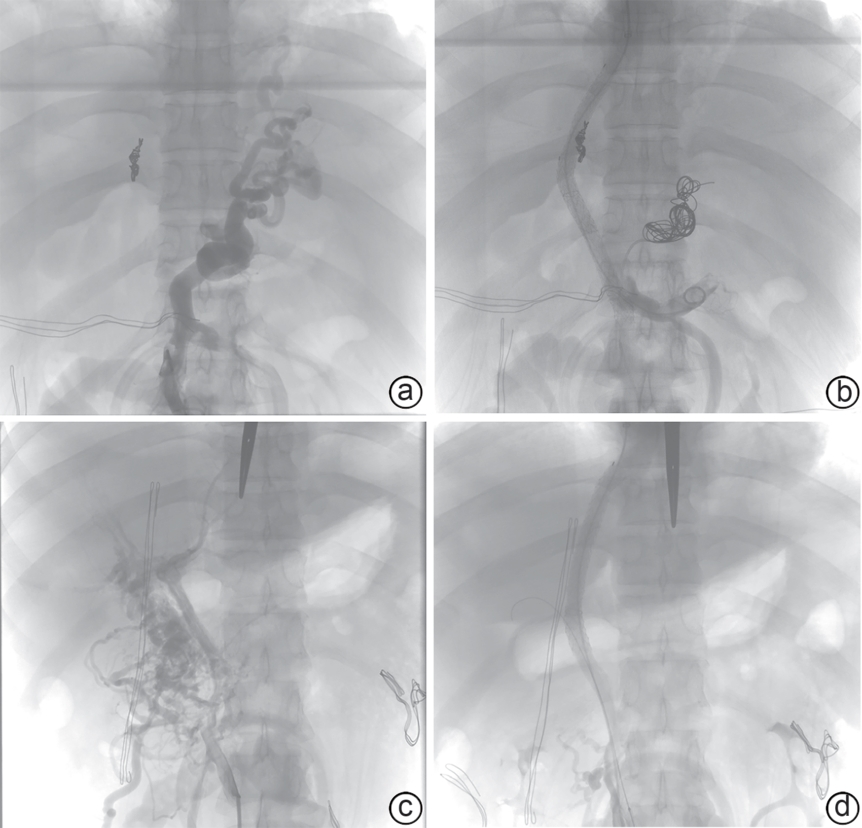
注: a、b,病例1,SA-TIPS分流前后数字减影血管造影,同期行胃冠状静脉栓塞,分流后未见食管胃底曲张静脉显影;c、d,病例2,SA-TIPS分流前后数字减影血管造影,分流后紊乱的侧支血管减少,提示分流有效且充分。SA-TIPS,外科辅助经颈静脉肝内门体分流术。
图 3 SA-TIPS分流前后数字减影血管造影
Figure 3. Digital subtraction angiography pre and post SA-TIPS
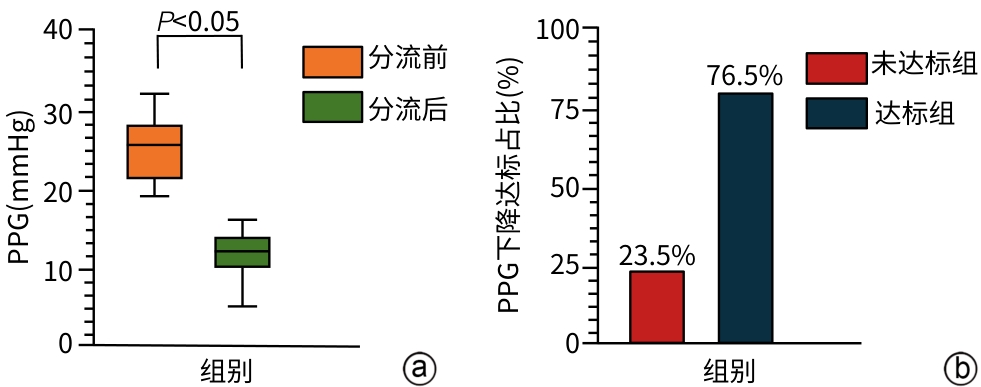
注: a,SA-TIPS分流前后PPG即时压力变化;b,即时PPG下降程度达标占比。SA-TIPS,外科辅助经颈静脉肝内门体分流术;PPG,门静脉压力梯度。
图 4 SA-TIPS分流前后PPG变化和分流达标率占比
Figure 4. Changes in PPG and the proportion of shunt
表 1 患者一般情况
Table 1. Basic characteristics of patients
项目 数值 男[例(%)] 20(55.6) 年龄(岁) 56(43~61) 病因 肝硬化[例(%)] 27(75.0) 乙型肝炎肝硬化[例(%)] 11(30.6) 丙型肝炎肝硬化[例(%)] 2(5.6) 酒精性肝硬化[例(%)] 4(11.1) 原发性胆汁性胆管炎[例(%)] 1(2.8) 自身免疫性肝硬化[例(%)] 2(5.6) 不明原因肝硬化[例(%)] 7(19.4) 非肝硬化[例(%)] 9(25.0) 肝移植后再发门静脉血栓[例(%)] 1(2.8) 阵发性睡眠性血红蛋白尿[例(%)] 1(2.8) 骨髓纤维化[例(%)] 1(2.8) 脐带感染病史[例(%)] 2(5.6) 其他[例(%)] 4(11.1) TIPS主要指征 EGVB[例(%)] 1(2.8) EGVB的二级预防[例(%)] 25(69.4) 顽固性腹水[例(%)] 4(11.1) 顽固性胸腔积液[例(%)] 4(11.1) 慢加急性血栓形成[例(%)] 2(5.6) 是否合并肿瘤 不合并肿瘤[例(%)] 29(80.6) 合并肿瘤[例(%)] 7(19.4) 原发性肝癌[例(%)] 4(11.1) 胆管癌[例(%)] 1(2.8) 继发性肝癌[例(%)] 1(2.8) 其他肿瘤[例(%)] 1(2.8) 腹腔手术史 无外科手术史[例(%)] 24(66.7) 有外科手术史[例(%)] 12(33.3) 脾切除术[例(%)] 5(13.9) 胆囊手术[例(%)] 2(5.6) 阑尾切除术[例(%)] 2(5.6) 疝气手术[例(%)] 2(5.6) 肠管切除[例(%)] 1(2.8) 术前检验 白细胞计数(×109/L) 3.94(2.65~5.19) 血小板计数(×109/L) 71.5(52.0~142.5) 血红蛋白(g/L) 82.5(69.0~90.0) Child-Pugh评分(分) 8(6~9) Child-Pugh分级[例(%)] A级 14(38.9) B级 16(44.4) C级 6(16.7) 注:TIPS,经颈静脉肝内门体分流术;EGVB,食管胃底静脉曲张破裂出血;Child-Pugh评分/分级,蔡尔德-皮尤评分/分级。
 下载: 导出CSV
下载: 导出CSV
表 2 SA-TIPS的手术实施情况
Table 2. The implementation details of SA-TIPS
项目 数值 分流结果 成功[例(%)] 34(94.4) 未成功[例(%)] 2(5.6) 同期手术 食管胃底静脉栓塞术[例(%)] 15(41.7) 门静脉放射性125I粒子条置入术[例(%)] 1(2.8) 下腔静脉滤器置入术[例(%)] 1(2.8) 穿刺针数 1.7±0.9 1次[例(%)] 18(50.0) 2次[例(%)] 11(30.6) 3次[例(%)] 4(11.1) >3次[例(%)] 3(8.3) 分流道近端位置 肝右静脉[例(%)] 9(26.5) 肝中静脉[例(%)] 10(29.4) 下腔静脉[例(%)] 15(44.1) 分流道远端位置 脾静脉[例(%)] 9(26.5) 肠系膜上静脉[例(%)] 10(29.4) 门静脉主干远端[例(%)] 12(35.3) 门静脉主干近端[例(%)] 3(8.8) 分流道长度(cm) 11.0±2.6 支架植入数量 1枚[例(%)] 13(38.2) 2枚[例(%)] 21(61.8) 复查超声流速 平均流速(cm/s) 121.7±35.2 峰值流速(cm/s) 133.1±41.9 手术时间(h) 4.3±1.1 透视时间(min) 42.7±7.5 累积空气比释动能(mGy) 2 177.5±821.7 拔除气管插管 术后即刻拔除[例(%)] 21(58.3) 转监护室后拔除[例(%)] 15(41.7) 注:SA-TIPS,外科辅助经颈静脉肝内门体分流术。
下载: 导出CSV
表 3 围手术期并发症
Table 3. Perioperative complications
并发症 数值[例(%)] 处理 结果 心律失常 室上性心动过速 1(2.8) 停止腔内操作并观察 片刻后恢复心率 房颤 1(2.8) 停止腔内操作并观察 恢复心率 出血 胸腔出血 1(2.8) 术后胸腔引流,应用止血药物 血红蛋白逐渐平稳 腹腔出血 2(5.6) 止血、补液、输血 术后腹腔引流均逐渐减少,无血性液体 感染 系统感染 0(0.0) 预防性应用抗生素 切口感染 1(2.8) 清创再缝合 切口愈合良好
下载: 导出CSV
-
[1] European Association for the Study of the Liver. EASL clinical practice guidelines on TIPS[J]. J Hepatol, 2025, 83( 1): 177- 210. DOI: 10.1016/j.jhep.2025.01.029. [2] The Chinese College of Interventionalists. CCI clinical practice guidelines: Management of TIPS for portal hypertension(2019 edition)[J]. J Clin Hepatol, 2019, 35( 12): 2694- 2699. DOI: 10.3969/j.issn.1001-5256.2019.12.010.中国医师协会介入医师分会. 中国门静脉高压经颈静脉肝内门体分流术临床实践指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35( 12): 2694- 2699. DOI: 10.3969/j.issn.1001-5256.2019.12.010. [3] ZHANG JB, CHEN J, ZHOU J, et al. Systematic review and meta-analysis of trans-jugular intrahepatic portosystemic shunt for cirrhotic patients with portal vein thrombosis[J]. World J Clin Cases, 2021, 9( 19): 5179- 5190. DOI: 10.12998/wjcc.v9.i19.5179. [4] RODRIGUES SG, SIXT S, ABRALDES JG, et al. Systematic review with meta-analysis: Portal vein recanalisation and transjugular intrahepatic portosystemic shunt for portal vein thrombosis[J]. Aliment Pharmacol Ther, 2019, 49( 1): 20- 30. DOI: 10.1111/apt.15044. [5] VALENTIN N, KORRAPATI P, CONSTANTINO J, et al. The role of transjugular intrahepatic portosystemic shunt in the management of portal vein thrombosis: A systematic review and meta-analysis[J]. Eur J Gastroenterol Hepatol, 2018, 30( 10): 1187- 1193. DOI: 10.1097/MEG.0000000000001219. [6] GUO DF, FAN LW, LE Q, et al. Transjugular intrahepatic portosystemic shunt for the prevention of rebleeding in patients with cirrhosis and portal vein thrombosis: Systematic review and meta-analysis[J]. Front Pharmacol, 2022, 13: 968988. DOI: 10.3389/fphar.2022.968988. [7] ZHU KS, MENG XC, ZHOU B, et al. Percutaneous transsplenic portal vein catheterization: Technical procedures, safety, and clinical applications[J]. J Vasc Interv Radiol, 2013, 24( 4): 518- 527. DOI: 10.1016/j.jvir.2012.12.028. [8] SALEM R, VOUCHE M, BAKER T, et al. Pretransplant portal vein recanalization-transjugular intrahepatic portosystemic shunt in patients with complete obliterative portal vein thrombosis[J]. Transplantation, 2015, 99( 11): 2347- 2355. DOI: 10.1097/TP.0000000000000729. [9] LI WX, CUI MZ, LI Q, et al. Application of transmesenteric vein extrahepatic portosystemic shunt in treatment of symptomatic portal hypertension with cavernous transformation of portal vein[J]. J Interv Med, 2023, 6( 2): 90- 95. DOI: 10.1016/j.jimed.2023.04.001. [10] JALAEIAN H, TALAIE R, D’SOUZA D, et al. Minilaparotomy-assisted transmesenteric-transjugular intrahepatic portosystemic shunt: Comparison with conventional transjugular approach[J]. Cardiovasc Intervent Radiol, 2016, 39( 10): 1413- 1419. DOI: 10.1007/s00270-016-1385-3. [11] LI HJ, YIN FQ, MA YT, et al. Administration of anticoagulation strategies for portal vein thrombosis in cirrhosis: Network meta-analysis[J]. Front Pharmacol, 2025, 15: 1462338. DOI: 10.3389/fphar.2024.1462338. [12] ZHU JY, XIA YF, LIU X, et al. Preventing variceal rebleeding in cirrhotic patients with portal vein thrombosis: A systematic review and meta-analysis[J]. J Gastroenterol Hepatol, 2024, 39( 4): 642- 648. DOI: 10.1111/jgh.16489. [13] SUN GL, WANG JY, ZHANG BN, et al. Case report: Management of liver cancer complicated by gastric varices rupture and bleeding: Transjugular intrahepatic portosystemic shunt utilizing the mesenteric venous pathway[J]. Front Med, 2024, 11: 1388584. DOI: 10.3389/fmed.2024.1388584. [14] PELIZZO G, QUARETTI P, MORAMARCO LP, et al. One step minilaparotomy-assisted transmesenteric portal vein recanalization combined with transjugular intrahepatic portosystemic shunt placement: A novel surgical proposal in pediatrics[J]. World J Gastroenterol, 2017, 23( 15): 2811- 2818. DOI: 10.3748/wjg.v23.i15.2811. [15] DAVIS JPE, LIM JK, FRANCIS FF, et al. AGA clinical practice update on management of portal vein thrombosis in patients with cirrhosis: Expert review[J]. Gastroenterology, 2025, 168( 2): 396- 404. DOI: 10.1053/j.gastro.2024.10.038. [16] LYU Y, FAN DM, HAN GH. Application status and future prospect of transjugular intrahepatic portosystemic shunt in gastroesophageal variceal bleeding in liver cirrhosis[J]. J Clin Hepatol, 2022, 38( 6): 1229- 1233. DOI: 10.3969/j.issn.1001-5256.2022.06.004.吕勇, 樊代明, 韩国宏. 经颈静脉肝内门体分流术在肝硬化食管胃底静脉曲张破裂出血中的应用现状与未来展望[J]. 临床肝胆病杂志, 2022, 38( 6): 1229- 1233. DOI: 10.3969/j.issn.1001-5256.2022.06.004. [17] LI TQ, LIU JC, ZHOU C, et al. The auxiliary target means used for improving the success rate of TIPS in treating portal vein occlusion[J]. J Interv Radiol, 2022, 31( 8): 805- 809. DOI: 10.3969/j.issn.1008-794X.2022.08.014.李铜强, 刘家成, 周晨, 等. 提高经颈静脉肝内门体分流术治疗门静脉闭塞技术成功率的辅助靶标手段[J]. 介入放射学杂志, 2022, 31( 8): 805- 809. DOI: 10.3969/j.issn.1008-794X.2022.08.014. [18] Hepatobiliary Disease Study Group, Chinese Society of Gastroenterology, Chinese Medical Association. Consensus for management of portal vein thrombosis in liver cirrhosis(2020, Shanghai)[J]. J Clin Hepatol, 2020, 36( 12): 2667- 2674. DOI: 10.3969/j.issn.1001-5256.2020.12.007.中华医学会消化病学分会肝胆疾病学组. 肝硬化门静脉血栓管理专家共识(2020年, 上海)[J]. 临床肝胆病杂志, 2020, 36( 12): 2667- 2674. DOI: 10.3969/j.issn.1001-5256.2020.12.007. [19] GIRI S, SINGH A, DAS S, et al. Efficacy and safety of transjugular intrahepatic portosystemic shunt in patients with hepatocellular carcinoma-a systematic review and meta-analysis[J]. Indian J Gastroenterol, 2024, 43( 6): 1121- 1135. DOI: 10.1007/s12664-024-01646-7. -

 本文二维码
本文二维码
计量
- 文章访问数: 335
- HTML全文浏览量: 133
- PDF下载量: 106
- 被引次数: 0

